Diabolical MERS-derived, “Chimera” Coronavirus Masquerading as the ‘Common Cold’?
The First Jar—Painful Sores
Then I heard a loud voice coming from the house of God. The voice said to the seven angels, “Go and pour out the seven jars of God’s anger onto the earth!”The first angel poured out his jar of God’s anger onto the earth. Painful sores were given to everyone who had the mark of the
wild animaland who worshiped his god — Revelation 16:1–2 NIV
Armstrong’s Apocalypse Illustrated
The year 1975 in prophecy
The 666 Symbol¹
¹ That’s one of the best reasoning I’ve read for the underlying meaning and numerology of 666. Tangentially I cited another possible meaning in my blog Legacy Bitcoin Rises Surreptitiously as the Reserve in a new Two-tier Monetary System; whilst impostor Bitcoin Core Dies:
[2]The likely meaning of “666” is submission to the will (2/3 quorum) of the super-majority in politics, governance, mass mania, etc.. Refer toMatthew 22:21,1 Samuel 8,John 15:19andRevelation 18:4. Whereas,Romans 13:1appears to be an integral part of the 666 system (perhaps a corrupted translation instituted by Constantine?).
Biblical Plagues?
Threat to Agriculture [Due to] Climate Cooling:
When we look at the plague of locust in Africa which is now spreading to China, it brings up visions of the Book of Exodus, which recounts around 1446 BC the Egyptians experienced an exceptional ravenous Plague of Locusts which was the eighth Biblical plague:
“They covered the face of the whole land, so that the land was darkened, and they ate all the plants in the land and all the fruit of the trees that the hail had left. Not a green thing remained, neither tree nor plant of the field, through all the land of Egypt.”
[…]
Pestilence in the northwestern provinces of China during 311 AD resulted in the death of 98% of the population. They blamed the crisis on locusts.
There was a link also with the rise in the population of rats that spread disease since they devoured the locust carcasses.[And the Black Death originated from Asia]
[…]
From a cyclical perspective, using the data from China, there were 116 major outbreaks over a period of nearly 2000 years. The average plague event seemed to be 17.2 years […] A recent study shows that locust swarms in China align with periods of climate turning colder […]
Four Horsemen of the Apocalypse

Death on the Pale Horse, 1796
The Insane Clusterfuck of the Collapse of Rule-of-law, Eventually to Imprison Most Westerners is an example of the warning in 1 Samuel 8 of what happens to those who w(h)or(e)ship government instead of the Lord as their King.
Contrast the acceleration since The Ten Plagues That Are Hitting America Right Now in 2014 to 10 ‘Plagues’ That Are Hitting Our Planet Simultaneously in 2020.
China Warns Of Looming “Locust Invasion” As Coronavirus Outbreak Fades:
Is the world’s largest constitutionally atheist state facing a revival of the 10 biblical plagues of Egypt? […] Just days after Beijing promised to send a 1,000-duck “army” to Pakistan…
each adult can consume the equivalent of its own weight in food every 24 hours […]
“A swarm the size of Rome can eat enough food in one day as everybody in Kenya.”
A Plague Of “Billions” Of Locusts Threatens To Create Horrific End-Times Famine Across Africa:
a single locust swarm can have “up to 150 million locusts per square kilometer”
[…]
In fact, one of the largest swarms in northeastern Kenya was measures to be “60 kilometers long by 40 kilometers wide”
[…]
this plague of locusts
could get“500 times”larger when warmer weather arrives
Clinical Novelty of the New Coronavirus
Widespread asymptomatic and/or mild symptoms , early-in-onset transmission would be a critically pertinent distinction between the original SARS (SARS-CoV) and the new SARS-CoV-2 virus².
Because it wouldprecludethe containment that prevented SARS (and Ebola) from becoming pandemics.
asymptomatic \ ˌā-ˌsim(p)-tə-ˈma-ti-k \
adjective. (of a disease or suspected disease) without symptoms; providing no subjective evidence of existence.
Note COVID-19 is the name of the respiratory disease caused by the SARS-CoV-2 virus.
² Previously known as the 2019 ‘novel coronavirus’ aka ‘2019-nCov’ and hereto referred to as ‘nCov-19’ for brevity:
Why do the virus and the disease have different names?
Viruses, and the diseases they cause, often have different names. For example, HIV is the virus that causes AIDS. People often know the name of a disease, such as measles, but not the name of the virus that causes it (rubeola).
Hmm. Is the WHO expecting there to be an important distinction between the viral infection (analogous to HIV) and the disease (analogous to AIDS)?
Evidence of Asymptomatic and/or Mild Symptoms, Early Transmission
Consensus Document on the Epidemiology of SARS:
There are currently no reports of the transmission of SARS from asymptomatic individuals.
UK businessman asymptomatically infected 11 persons and perhaps many more:
He said he contacted his GP, NHS 111 and Public Health England, on learning he had been exposed to a confirmed case of coronavirus.
He added: “I was advised to attend an isolated room at hospital, despite showing no symptoms
A Person Can Carry And Transmit COVID-19 Without Showing Symptoms, Scientists Confirm
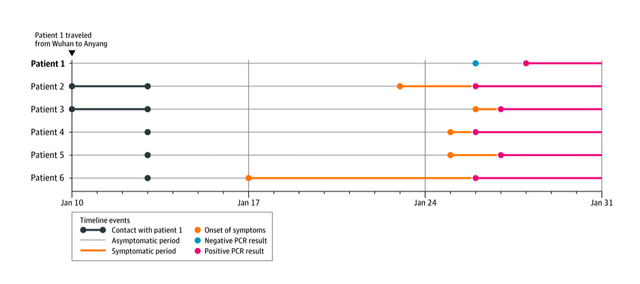
The case study is
the first[another] concrete evidence that a person showing no symptoms can pass the coronavirus to others [with a negative RT-PCR pre-transmission and positive test result post-transmission] — a fact that could make curbing the outbreak even more challenging.
[…]
For now, the woman’s asymptomatic transmission appears to be an anomaly, but health experts have documented other instances in which people tested positive for the virus without showing symptoms.
A report from the Chinese Centre for Disease Control and Prevention analysed records of all of China’s reported cases of the virus from December 8 to February 11 and found that
1.2 percent of patients confirmed to be infected showed no symptoms. [←very few asymptomatic patients were tested, so that actual percentage of those infected in the population-at-large is presumably much higher]A far higher portion of asymptomatic cases was found on the Diamond Princess cruise ship, where
322 of 621 people tested positive but showed no symptoms.
The ostensibly disinformation, hullabaloo, “Study claiming new coronavirus can be transmitted by people without symptoms was flawed” seems to misrepresent the totality of the Study documents first case of coronavirus spread by a person showing no symptoms, because it focused only on the extremely mild symptoms of the Index Patient and fails to even mention that Patient 1 apparently asymptomatically transmitted to Patients 3 and 4 during the incubation period. And the transmission to at least Patient 3 was 3–4 days before the onset of symptoms and only 1 day after Patient 1 presumably acquired the infection from the Index Patient!
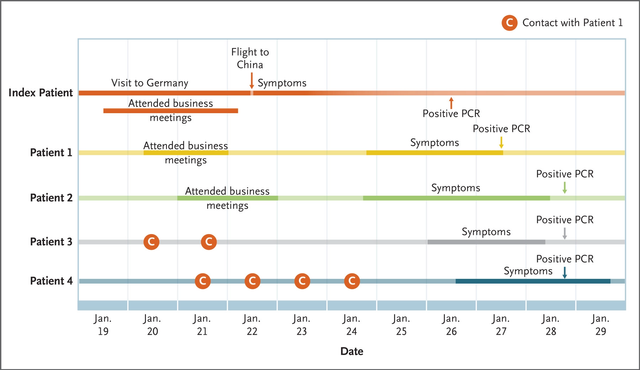
Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany
Even if we presume that somehow the Index Patient transmitted the infection to Patient 3 indirectly (they never met), one of the authors makes a point which may be even more pertinent than purely asymptotic transmission:
The German cluster does reveal another interesting aspect about the new virus, Drosten says. So far most attention has gone to patients who get seriously ill, but all four cases in Germany had a very mild infection. That may be true for many more patients, Drosten says, which may help the virus spread. “There is increasingly the sense that patients may just experience mild cold symptoms, while already shedding the virus,” he says.
“Those [mild symptoms] are not symptoms that lead people to stay at home.”
Additionally no where is it claimed the Index Patient was coughing and sneezing when she attended the business meeting with Patient 1. So WHO misrepresents the risk:
But even if they do, asymptomatic transmission likely plays a minor role in the epidemic overall, WHO says. People who cough or sneeze are more likely to spread the virus
Thirteen additional infections spawned from the aforementioned infected patients with mild symptoms.
The Chinese are staying at home but most Westerners are blissfully going about spreading the virus and not knowing it:

Inside China: […]
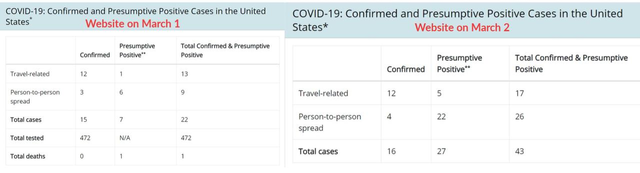
Did CDC Stop Disclosing How Many Americans Are Being Tested For Covid-19?

The Global Times, meanwhile, is now mocking the CDC [and WHO] for refusing to recommend that Americans should wear facemasks.
[…]
the CDC has stopped disclosing the number of Americans tested for coronavirus
[…] “The lack of testing is a scandal…This is the coverup.”
The United States badly bungled coronavirus testing
“I Have To Plead For Tests” - NYC ER Doc Warns “There's Going To Be 1000s Of US Cases By Next Week”:
The CDC sent test kits earlier in the outbreak to public health labs around the country, but those kits were problematic and potentially inaccurate […] says he still does not have access to test kits […] “I still have to make my case, plead to test people
Govt Forced Days Delays in Testing Patients With Symptoms
CDC Refused to Test “Patient Zero” Apple Co-Founder Steve Wozniak in early January, c.f. also
1000s Wait For Hospital Beds In South Korea, US Test Shortage Forces Patients To “Sweat It Out”
Novel Corona virus SARS-CoV-2 and technological decay:
Inability to produce test kits […] indicates an absolute decline in critical technology in the US
[…]
China used ten year old technology to develop test kits for SARS-CoV-2 in a few days, and now has millions of test kits.
Australia and Singapore have an adequate supply of locally produced test kits, with which they appear to be successfully controlling the spread. Everyone coming in at the airport with a fever gets tested, even if they do not have dry cough or diarrhea, everyone exposed to someone with corona virus gets tested.
In America, almost every case that has been detected among people who have not been overseas has been detected in people who are very seriously ill. Which tells me that there is no testing on contact tracing
[…]
The west has lost its nuclear technology. We cannot make Plutonium 238 any more […] Our [newest] fighter planes cannot fly as high, as far, or as fast
In New data from China buttress fears about high coronavirus fatality rate, WHO expert says:
Bruce Aylward, who led an international mission to China to learn about the virus and China’s response, said the specialists did not see evidence that a large number of mild cases of the novel disease called Covid-19 are evading detection […] Aylward pointed to an analysis from Guangdong […] worried people flooded fever clinics to be tested. Of 320,000 tests performed, just
under 0.5%[exactly 0.47% on pg 9³] were positive for the virus at the peak of transmission there, he said — which suggests that only 1 case out of 200 was being missed.
At that juncture the official count of cumulative, confirmed infection was 0.0084% of Hubei’s population. Citing a statistic from Guangdong is intentionallymisleading because the hospital system was most overwhelmed and thus unable to test everyone in Hubei. On the February 16 date of the WHO report³, Hubei had 44X more cases and has half the population compared to Guangdong. The official disparity continued to rise to 50X as of March 6 increasing from 14X at the juncture of the quoted 0.47% statistic.
From anecdotal reports and common sense, we know that the hospital system in Wuhan was refusing mild cases until at least February 5 when the exhibition center began accepting patients. Presuming all of the mild and a third of the moderate (c.f. pg 12³) were refused testing at the juncture of the quoted statistic then perhaps actual infections were ~1 ÷ 0.3 = 3.33 times officially reported. Thus ~14X × 3.33 = 47X and 47 × 3.33 = 16,327 cases which is roughly aligned with “suspected cases”. As China opened massive new makeshift hospitals for mild cases, official reporting may or may not have improved statistically because the case load may have been increasing much slower in Guangdong due to quarantine of Hubei. And the percentage of very mild cases may be skewed by mild patients being refused testing and/or mild patients not bothering to go to the hospital given the presumed high incidence of respiratory ailments in Wuhan (c.f. also SO₂ pollution satellite image below), difficulty of travel in the lockdown, fear of nosocomial infection, internment or overwhelmed hospitals. Also there’s the false negative rate as high as 50–70% perhaps due to swabbing in the throat instead of the nose per research cited below?
It seems plausible that China missed 80 - 90% of the infections. Thus estimated total infections in China as of March 7 would be ~0.7 million. Actual case fatality rate (CFR) would be ~0.5% unless (as alleged from anecdotal reports) China is—as its historical practice suggests—also underreporting deaths. Excellent healthcare may significantly lower CFR given it’s currently 0.6% in S. Korea, 0.0% in Singapore and 0.8% for the Diamond Princess where there has been ostensibly much more rigorous testing.

Tencent briefly lists 154,023 infections and 24,589 deaths
Why would China quarantine 114 million people if there were only the several hundred officially reported deaths at that juncture?
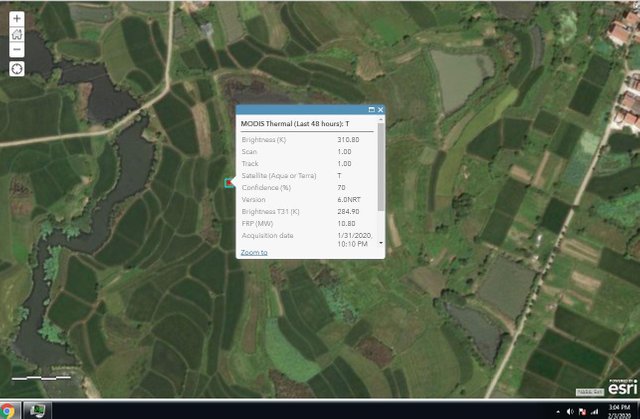
“theres a ‘metric f*ckton o’carcasses’”

“open-pit mongolian bbq”
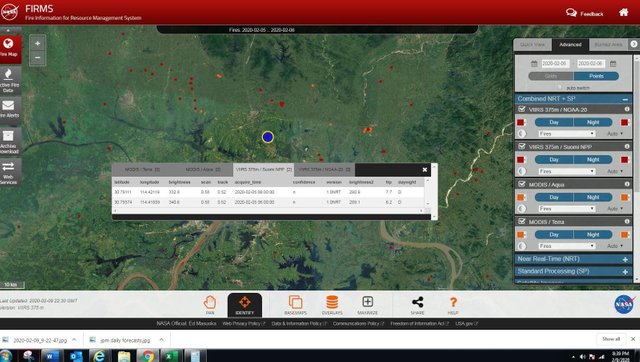
“Human [SO₂] Offgassing from Chinese BBQ Spareribs”
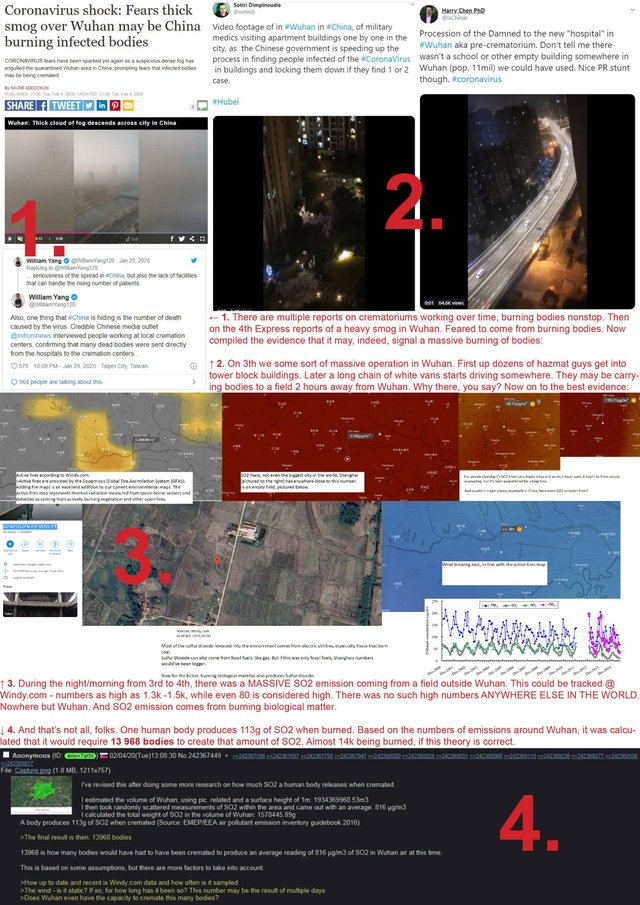
evidence of over 13k bodies being burned in an empty field
I won’t presume incompetence where malice (such as vested interest in pandemic bonds?) is only the plausible explanation. Maybe it’s a globalist The reproducibility crisis leftist singularity embraced by the CDC and the WHO Director-General:
So — According to Tedros, travel restrictions might lead to panic and racism […] “Obviously […] the virus doesn’t discriminate based on race. Why do we?”
The following is myopic because even just the alleged an order-of-magnitude lower than truth (c.f. also) official infection rate (unless it could be significantly reduced with infection control) will overwhelm the healthcare capabilities of any nation, including the USA:
But if there aren’t large numbers of uncounted cases, the [COVID-19 disease] severity seen in China is what the rest of the world should expect as the virus moves to new locations, especially if it spreads to the degree seen in Hubei province, where the outbreak began.
Fauci Warns Outbreak Could Overwhelm US Health-Care System:
Dr. Fauci says [15–]20% of Covid-19 cases could require hospitalization
[…]
Pence ended his latest briefing by claiming “the risk of the coronavirus to the average American remains low,” then walked off w/o answering
[…]
Jesus, the outbreak around Seattle was only found bc enterprising researchers found a way to get around the CDC.
INTRoDuCiNG THe PaNDeMiC BRoTHeRS...

Many mild infections are typically not reported and […] may support stealth transmission […] We estimate
86% of all infections were undocumented[…in Wuhan…] were 52% as contagious as documented infections […]source of infection for [⅔] of documented cases. Our estimate of the [R₀] (2.23; [1.77-3.00]) aligns with earlier findings; however, after travel restrictions and control measures were imposed this number falls considerably.
Reporter’s Notebook: Life and death in a Wuhan coronavirus ICU:
I often cried because so many patients could not be admitted […]
They wailed in front of the hospital. Some patients even knelt down to beg […] all beds were occupied.I shed tears while I turned them down. I ran out of tears now. I have no other thoughts but to try my best to save more lives.
[…]
You had to have had exposure to the South China Seafood Market, […] to have had a fever and test positive for the virus […] to meet all three criteria in order to be diagnosed […] In reality,
very few people were able to [even] test for a virus.
…South Korea Reports Huge Jump In New Cases: Virus Updates:
1900 Shincheonji Church members have been tested […] 1300 had symptoms & 600 did not. Among those 1300 with symptoms, 87.5% were confirmed with the virus […]
of the 600 WITHOUT symptoms, 70% were confirmed with coronavirus.
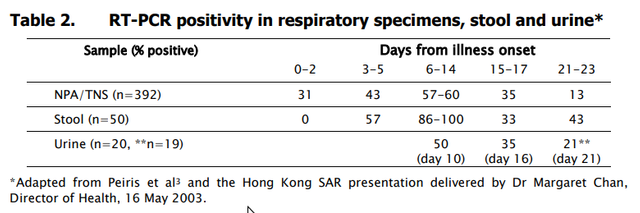
SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients
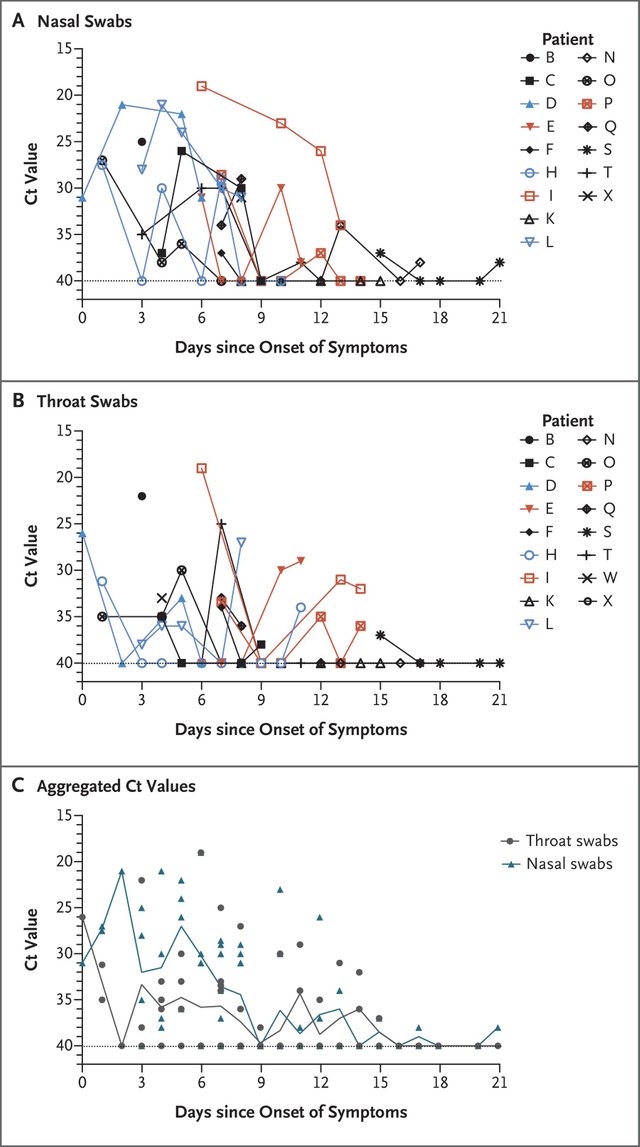
We analyzed the viral load in nasal and throat swabs obtained from the 17 symptomatic patients in relation to day of onset of any symptoms (Figure 1C).
Higher viral loads(inversely related to Ct value)were detected soon after symptom onset, with higher viral loads detected in the nosethan in the throat. Our analysis suggests that the viral nucleic acidshedding pattern of patients infected with SARS-CoV-2 resembles that of patients with influenza and appears different from that seen in patients infected with SARS-CoV. The viral load that was detected in theasymptomatic patient was similar to that in the symptomaticpatients, which suggests the transmission potential of asymptomatic or minimally symptomatic patients. These findings are in concordance with reports that transmission may occur early in the course of infection
What we know about the locally transmitted coronavirus cases in Singapore:
Case 19 [her workplace visited by the Chinese tour…] reported having a sore throat and fever on Jan 29 […] Case 21 is case 19’s domestic helper […] reported onset of symptoms on Feb 2
[…]
Case 20 [ a colleague of case 19…] reported onset of symptoms on Jan 25
[…]
Case 24 is a 32-year-old Singaporean[…] tour guide […]
had no symptomswhen she went to NCID on Feb 3
husband of a 32-year-old tour guide […] first reported that he developed a fever on Jan 24
Untraceable coronavirus cells emerge in three countries amid pandemic:
Doctors fear the spread could quicken and widen if they are unable to identify all those infected and get them into quarantine. Making matters worse, coronavirus symptoms are often so mild that a spreader could be unaware they are infected.
Coronavirus outbreak edges closer to pandemic status:
The novel coronavirus may be particularly suited for stealth community transmission since its
symptoms can be indistinguishable from those of a cold or the flu[…] Experts estimate it takes about a week for the number of infections in a given community to double […]it probably would take several weeks for a new infection cluster to be picked up by a local health department
Here Comes the Coronavirus Pandemic:
In the meantime, this much is not in dispute: SARS-CoV-2 spreads easily — more easily than SARS or seasonal flu — and is tough to detect.
Most coronavirus cases are mild, complicating the response:
about
82 percentof the cases — including all 14 in the United States —have been mild, with symptoms that require little or no medical intervention. And that proportion may be an undercount.
Why the coronavirus outbreak might be much bigger than we know:
The main method of screening for the disease in many countries is still testing passengers from China […] people carrying the virus from elsewhere may be undetected.
[…]
Until this week,
only two countries in Africa had the lab capacity to screen for this disease— Senegal and South Africa […] So far, not a single case has been detected in Africa — and Africa is thought to be at particular risk given its links to China
[…]
To understand Covid-19’s spread, scientists need what’s known as serology testing, Ryan said. With serology tests, health officials can
find out how many people developed antibodies to fight the virus by randomly sampling populations. This would detect all those mild or even asymptomatic cases that may be getting missed right now
“What I’ve learned in the last two weeks is […] There’s much more asymptomatic illness,” he added. “A number of the confirmed cases that we confirmed actually just presented with a little sore throat.”
Trump was not told coronavirus-infected Americans would be flown home from cruise ship
Diamond Princess: State Department flew coronavirus-infected Americans to the US against CDC advice
Whether the Basic reproduction number (R₀) for transmission of nCov-19 is significantly higher than for SARS, probably isn’t the salient issue, given it’s only a threshold whose absolute value is more of theoretical speculation because it may be modulated over time by numerous factors such as:
- Population density, c.f. also
- Focus of infection such as close contact with wild animals or domestic cats (c.f. also), or enclosed structures which propagate the virus through air-conditioning ducts or drain pipes (but not air-conditioning on airplanes although within 7 rows of proximate seating transmitted SARS).
- Infection control such as hygiene, vaccines, quarantines and travel restrictions
- Airborne respiratory viruses don’t spread as efficiently in climates with higher absolute humidity.⁴ Warmer air holds more water. A potentially slower growing reservoir due to slower spread can continue in the summer as was the case for the 1918 influenza “Spanish” flu, especially if it’s being continuously replenished by the most severely ill of the traveling soldiers stationed in a nexus of close quarters.
Note so far there’s no exponential community transmission of COVID-19 between the Tropics of Cancer and Capricorn, excepting focuses-of-infection and cold, high altitude climates. And it’s currently Summer in the Southern Hemisphere.
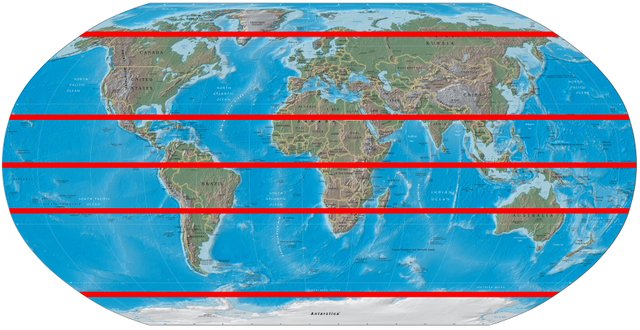
Although mild and asymptomatic cases of nCov-19 infection may be undetected, especially in these poor countries wherein most people don’t go to the doctor when they feel slightly ill unlike in the more affluent Singapore, the absence of reported deaths traced to community transmission in populous, impoverished S.E. Asia seems to indicate the transmission is significantly reduced in warm, humid climates, absent some other focus-of-infection.
Note post-infection, epidemiological factors causally correlated to increased risk of mortality from viruses, such as the following for COVID-19:
- male gender
- advanced age:
The virus has killed 79 people in Italy, all aged between 63 and 95 with underlying serious illnesses […73%] percent of the Italian population is over 65, making it the oldest in the world after Japan.
- comorbidity, such as diabetes, cardiovascular disease, immune disorders, cancer, etc.
- any prior history of smoking but not current Causasian smokers, c.f. also
(incidence of which varies statistically by country and gender) - but not ACE2
These factors may or may not significantly impact R₀ for a given virus.
³ Report of the WHO-China Joint Mission
on Coronavirus Disease 2019 (COVID-19)
⁴ Viruses are genetic material ¹⁄₁₀₀ₜₕ the size and lacking the reproductive machinery of a biological cell such as bacteria. Imagine the effect of attaching to a gallon-size droplet of water vapor could do to an airborne, swirling piece of toilet paper.
Reinfection/Vaccination-induced Dysfunctional, Auto-immunopathology
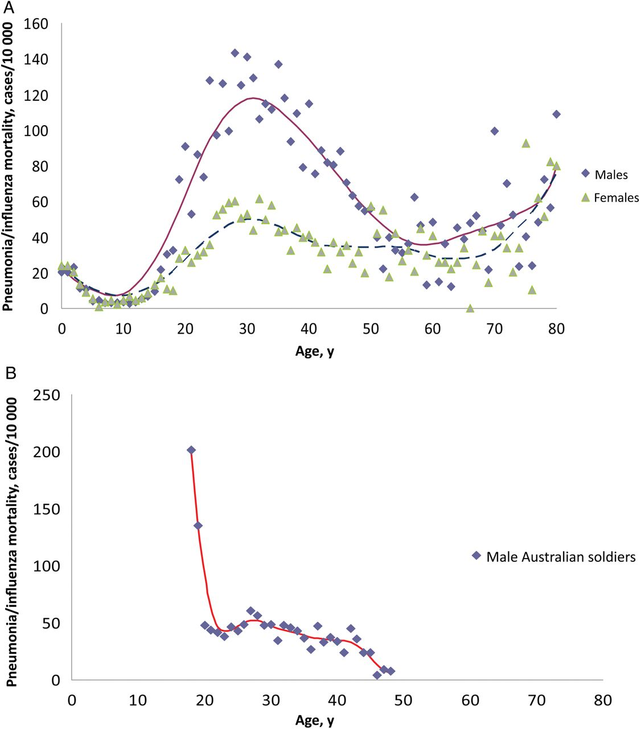
Conversely w.r.t. epidemiological factors, the more virulent second wave of 1918 influenza “Spanish” flu had increased mortality among youthful adults and the very young — presumably because the very young had no prior immunity to this highly virulent strain and the young adults may have had immunity to a H3 strain or timely reduction of H1 strain antibodies to the vulnerable titer range perhaps (and chart bell curve strongly suggestive of) leading to some dysfunctional mode of auto-immunopathology such as original antigenic sin (OAS) or antibody-dependent enhancement (ADE, c.f. also), whilst older adults may have had prior immunity to a relevant strain and/or depleted antibodies (to outside vulnerable titer range thresholds/parameters) precluding said dysfunctional immunopathology.
Lower mortality for females is not converse to coronaviruses SARS and COVID-19 (nCov-19), so presume same posited differential causal epidemiology plus presumably more male soldiers so perhaps the 1918 influenza virus natural-selected for male mortality (and possibly for the mortality of the average age of the cohort soldier combined with vulnerable antibody-dependent enhancement sweet spot cohort in that demographic). Mortality overall was also enhanced (presumably for all cohorts) by the lack of antibiotics in 1918 and thus additional cases of death by opportunistic bacterial pneumonia:
In civilian life, natural selection favors a mild strain. Those who get very ill stay home, and those mildly ill continue with their lives, preferentially spreading the mild strain. In the trenches, natural selection was reversed. Soldiers with a mild strain stayed where they were, while the severely ill were sent on crowded trains to crowded field hospitals, spreading the deadlier virus.
[…]
Older adults may have had partial protection caused by exposure to the 1889–1890 “Russian flu” pandemic.
[…]
most individuals born after 1900 would have had exposure to the original H1 virus, as children typically are infected with influenza by age 5 or 6 […] individuals who were born between 1880 and 1900 would have been exposed early to a different strain of flu, an H3 virus
[…]
The 1918 virus was at least 100 times more lethal than one of the other recombinant viruses tested
[…]
If a severe pandemic, such as occurred in 1918 happened today, it would still likely overwhelm health care infrastructure, both in the United States and across the world
[…]
The general form of age-specific mortality data in 1918, with a peak at a specific age, suggests that individuals were more or less susceptible to dying from influenza given their age at the time of the 1889–90 pandemic, rather than being more or less protected from earlier exposure to an antigenically similar virus. Since mortality peaks at age 28 in 1918, it seems straightforward to suppose that exposure during development and/or very early in life to the 1889–90 strain led to more severe response to infection in 1918.
Coronavirus Infections Outside Of China Are Growing Exponentially:
Also, new research provides the explanation for why those infected a second time by covid-19 are at much higher risk.
Chris breaks down the science in layman’s terms to explain the nature of the danger, but the key takeaway is: while you for sure don’t want to contract covid-19, you DEFINITELY don’t want to get it a second time…
Why Did the 1918 Virus Kill So Many Healthy Young Adults?
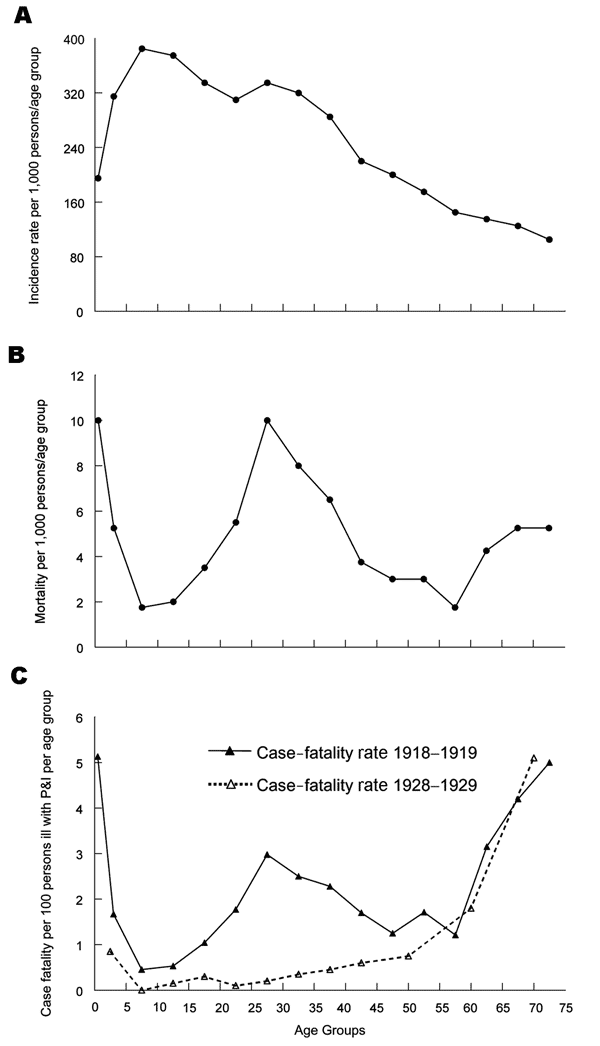
To explain this pattern, we must look beyond properties of the virus to host and environmental factors, possibly including immunopathology (e.g., antibody-dependent infection enhancement associated with prior virus exposures) and exposure to risk cofactors such as coinfecting agents, medications, and environmental agents.
Age-Specific Mortality During the 1918–19 Influenza Pandemic […]
Potential for ADE in nCov-19?
Chinese doctors say Wuhan coronavirus reinfection even deadlier:
It’s highly possible to get infected a second time. A few people recovered from the first time by their own immune system, but the meds they use are damaging their heart tissue, and when they get it the second time, the antibody doesn’t help but makes it worse, and they die a sudden death from heart failure.
Head of the National Institute of Allergy and Infectious Diseases (NIAID) at NIH, Dr. Fauci, denies the existence of the above:
During the 2009 influenza A(H1N1) pandemic,
several reports suggested prior vaccination with the 2008–2009 seasonal inactivated influenza vaccine increased severity of clinical diseasefollowing infection with the A(H1N1)pdm09 virus (Skowronski et al., 2010). The mechanism of vaccine-associated enhanced respiratory disease (VAERD) is not well understood. Using a swine model, Khurana et al. (2013) showed that vaccination of pigs with an H1N2 virus and challenge with a A(H1N1)pdm09 virus resulted in the pigs having enhanced pneumonia and disease.
Molecular mechanism for antibody-dependent enhancement of coronavirus entry: Discussions
ADE is also a major concern for vaccine design and antibody-based drugs therapy, since antibodies generated or used in these procedures may lead to ADE. ADE has been observed in coronavirus for decades […] In this study we first demonstrated that […] the same coronavirus strains that led to the production of fully neutralizing mAbs can be mediated to go through ADE by these neutralizing mAbs. Our results differ from previously observed ADE of flaviviruses [e.g. dengue] where primary infections and secondary infections are caused by two different viral strains and where ADE-mediating mAbs are only sub-neutralizing or non-neutralizing for secondary viral infections […] RBD-specific neutralizing mAbs mediate ADE of coronavirus entry by functionally mimicking viral receptors […] Importantly, ADE occurs only at intermediate mAb dosages. Our study explains an earlier observation where ADE of dengue viruses only occurs at certain concentrations [i.e. titers] of mAb […] ADE of viruses depends on antibody dosages, tissue-specific expressions of viral and Fc receptors, and some intrinsic features of the antibody […] different tissue cells should be closely monitored for potential ADE at certain antibody dosages […] Future research using in vivo systems is needed to further confirm these results […] the mechanism that we have identified for ADE of MERS-CoV in vitro may account for the
ADE observedin vivofor other coronaviruses such as SARS-CoVand feline coronavirus
The above indicates that theoretically reinfection of the related or same virus in some hosts (i.e. victims) with residual antibodies (from prior infection) of a certain types and titers, could cause the antibodies to mimic viral receptors and help the virus replicate in other types of cells than its normal pathway, such as for example other immune system cells, possibly causing an aberrant immune response in other tissues of the body such as for example blood vessels, nerve or neurological system. One could imagine any sort of strange outcomes such as encephalitis, Ebola-like hemorrhaging or sores all over the body.
Potential for OAS-induced Cytokine Storm in nCov-19?
SARS-CoV-2 Vaccine Recommended Readings
No, James Lyons-Weiler did not “break the coronavirus code”:
An early concern for application of a SARS-CoV vaccine was the experience with other coronavirus infections which induced enhanced disease and immunopathology in animals when challenged with infectious virus [31], a concern reinforced by the report that animals given an alum adjuvanted SARS vaccine and subsequently challenged with SARS-CoV exhibited an immunopathologic lung reaction […]”
Yes, in animal models, animals vaccinated with a SARS vaccine then challenged with the SARS coronavirus developed severe disease due to an excessive immune reaction to the virus primed by the vaccine. That is indeed a reason to be very cautious moving to clinical trials of vaccines against SARS, MERS, or 2019-nCoV.
[…]
whether this low homology match between the insert found in 2019-nCoV and pShuttle means that 2019-nCoV came from a failed Chinese effort to make a vaccine against SARS. Seriously […] Yes, Lyons-Weiler is actually suggesting that the Chinese sensitized their population with a SARS vaccine (which, he implies, was created using pShuttle-SN) and that the vaccine strain of virus escaped from the lab. He then seems to realize that that possibility would mean that this outbreak would likely be short and quickly contained, as there is
no evidence that China ever conducted a mass vaccination program against SARS, which would leave very few “sensitized” individuals.
Ahem. China with its high, international travel nexus and dic(k)tatorial culture would be the most ideal location for large-scale, surreptitious, human vaccine research (and possibly as the official excuse for compartmentalization of the involved, covert medical professionals, to prevent them from knowing what is really an intentional pump-priming for a well-timed pandemic serving the interests of the globalists).
Prison wardens of slave labor prisons who employ “comfortable torture chairs” (c.f. 1, 2) couldn’t be bribed or induced to allow vaccination experiments? Chinese prison population is 0.120% with 11 million population in Wuhan and 59 million for the Hubei province. It’s impossible that China’s total infections on Feb. 21 was ~500 as announced, implying an infection rate of only 1–4% of the ~13–71k prison population in the nexus of the outbreak’s quarantined hotbed. Infection would rapidly spread in the close quarters of prison (c.f. Epidemic Situation of Tuberculosis in Prisons in the Central Region of China) as it did for the Diamond Princess cruise ship. Instead China apparently waited to provide prison statistics just after they revised the criteria for “confirmed case” to be ~⅒ of diagnosed infections (not even factoring in the evidence of huge numbers of non-diagnosed mild, asymptomatic, home-bound or officially-ignored infections):
The specialists said that clinical symptoms really resembled SARS, but they were still talking about diagnosis criteria, that kind of stuff. We replied that those standards were too stringent. Very few people would get diagnosed based on those criteria. The head of our hospital told them this multiple times […] other hospitals were doing the same.
[…]
a new breakout[delayed reporting] was been observed in the local Hubei prison system
[…]
But wait, didn’t Hubei just change the definition of an “infection” to remove those cases confirmed with a CT scanner? Why is Wuhan rushing to add those scanners if their “confirmation” of a case is irrelevant?
The answer of course, is obvious: there is an order of magnitude more cases in Hubei - and China - than is officially reported
Absent compelling evidence that nCov-19 was accidentally created by vaccine research, there’s at least implicit evidence that vaccine research with spike proteins has been ongoing. And there’s circumstantial evidence (c.f. also) that nCov-19 could be a recombination of a PLA military “bat virus” with MERS and another less deadly human coronavirus that accounts for 10–15% of the annual cases of the common cold (more on this in a subsequent section). Conspiratorially vaccine research could be the covert pump-priming of an intentional, diabolical pandemic (and panic, forced vaccinations, forced quarantines[imprisonment], gun-control, political chaos, evisceration of economic confidence, scapegoat for the coming economic collapse, cashless economy, etc):
Current hypotheses include that a covert SARS vaccination program was included in the national mandatory vaccination program started on Dec 1, 2019 that happened to involve a secondary true outbreak of Coronavirus with secondary exposure
[…]
Another possibility is that a vaccine used by the Chinese has weakened their response to an otherwise mild coronavirus infection. SARS 2 binding to ACE2 is weaker. Thimerosal inhibits ERAP1. Vaccination with aluminum hydroxide containing vaccines might induce autoimmunity in the lungs. All of these factors could play a role in making vaccinated individuals more susceptible.
A third possibility is that people in that geographic region who had prior SARS infections might be less able to fight off SARS 2 simply due to original antigenic sin from infection. Toronto, Canada, take note.
Egregious SO₂ Air Pollution in Wuhan
And Wuhan an ideal location for pump-priming a pandemic?
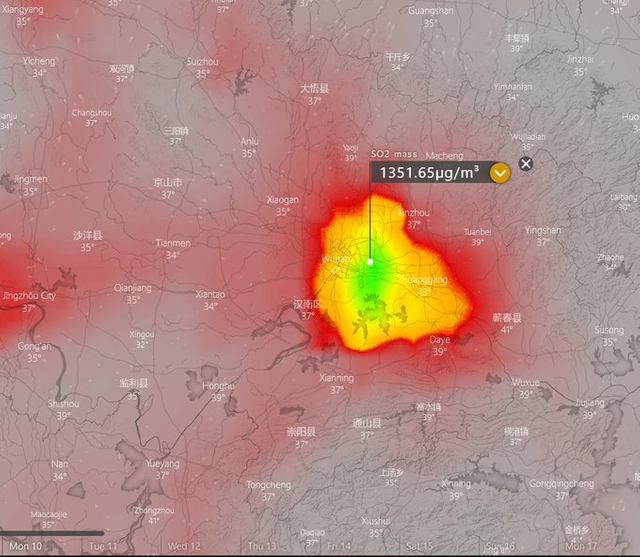
“there’s this enormous steel plant in the middle of the cloud...”
Typically factories work overtime in China before and after Chinese new year
Breathing in sulfur dust can irritate the airways or cause coughing.
Toxic Substances Portal - Sulfur Dioxide
Inhaled sulfur dioxide readily reacts with the moisture of mucous membranes to form sulfurous acid (H2SO3), which is a severe irritant.
[…]
Sulfur dioxide is severely irritating to the eyes, mucous membranes, skin, and respiratory tract. Bronchospasm, pulmonary edema, pneumonitis, and acute airway obstruction can occur. Inhalation exposure to very low concentrations of sulfur dioxide can aggravate chronic pulmonary diseases, such as asthma and emphysema.
China attempted to discredit without actually denying, lol:
China’s environment ministry has also rejected the claims, insisting that SO2 levels in Wuhan are normal […] “Sulphur dioxide readings in Wuhan were never higher than 11.5 µg/m3
in the week up to February 9”
Of course because they shut down the gimongous, steel factory.
Although highly speculative, there’s a non-zero risk of auto-immunopathology with nCov-19 reinfection (or potentially initial infection for those previously infected with other coronaviruses, influenza or their vaccines) considering:
- mortal COVID-19 usually involves cytokine storms in the lungs and sometimes whole body inflammation leading to sepsis, that has a notable hallmark of declining lymphocytes:
But those whose lymphocyte numbers continue to decline, those whose immune systems are destroyed in the end, experience multiple organ failure and die.
- reasonable hypothesis that dysfunctional immunopathology was the cause of the aberrant, egregious increase of mortality among the young adults for the 1918 “Spanish” influenza flu pandemic
- ADE observed in vivo for SARS, yet reinfections were presumably virtually non-existent in the wild because the epidemic was easily contained. Whereas, nCov-19 is likely to be an uncontainable pandemic with massive number of cases of multiple reinfections.
- peer reviewed genome and evolutionary virology evidence, speculatively and conspiratorially conjectured to support a hypothesis that nCov-19 was engineered for maximum long-term mortality, i.e. coupled with ongoing seasonal reinfection, mutation, vaccines, economic/climate deprivation cliff starting now — congruent with the [observed “engineering”] of the current, eugenics politics/ideology/societalcide enveloping the insane, decadent, clusterfucked West¹ — that irrationally accuses (especially white, patriarchal) man of destroying the planet and the stated ideological goal of the Georgia Guidestones:
- Maintain humanity under 500,000,000 in perpetual balance with nature.
Why I’m Ramping Up My Coronavirus Preparations:
In yesterday’s video (Coronavirus Infections Outside Of China Are Growing Exponentially) from Feb 19th, 2020, I put out the science behind why a second exposure may be worse than the first. That’s anything but proven at this point, but the fact that both SARS and MERS are that way, and given the high degree of sequence homology between both of those and COVID-19 we’re just going to have to guess that a second exposure to COVID-19 is worth avoiding.
So much so that I’ve made the personal decision that I’m not going to get it the first time around. Mostly to avoid being at risk of getting it a second time.
That’s a calculation based on the currently available data, which, admittedly, involves making a number of assumptions and a couple of educated leaps.
I’m uncomfortable speculating in public because I’d be crucified by those protecting the official narrative.
Here’s my primary personal strategy when it comes to the coronavirus (aka covid-19):
Don’t get infected!
Uncontainable
We’re Close To Your Last Day To Prepare For The Coronavirus:
The coronavirus has probably been spreading undetected for about six weeks [direct link] in Washington state, where the first U.S. death was reported this weekend, according to new research. A genetic analysis suggests that the cases are linked through community transmission and that the virus is likely to have been spreading undetected for weeks, with hundreds of infections possible in the state:
“This strongly suggests that there has been cryptic transmission in Washington state for the past 6 weeks,”
Implying there’s already thousands of infections in the U.S.A.:
Former FDA Director Scott Gottlieb [a Republican, Trump appointee…] warned that the number of cases in the US has probably already reached the ‘low thousands’. Hundreds could be confirmed by the end of the week.
The implausibility of detecting and isolating patients that become highly contagious either in the incubation period or very soon after only mild flu-like symptom implies that without a vaccine, nCov-19 infection will be a pandemic that eventually (perhaps within one or two more winters) spreads to a majority of the population of the world — at least for arid or cold regions.
Conversely, SARS was containable because patients were only contagious after nearly a week following initial symptoms and highly contagious only when experiencing detectable, distinguishable, deteriorating symptoms:
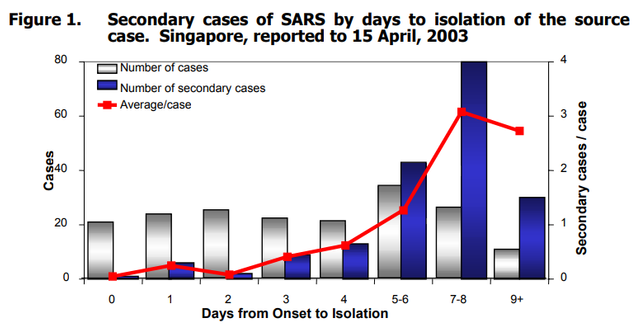
Consensus document on the epidemiology of SARS: Infectious period
Transmission efficiency appears to be greatest from severely ill patients or those experiencing rapid clinical deterioration, usually during the second week of illness. Data from Singapore (Figure 1) show that few secondary cases occur when symptomatic cases are isolated within 5 days of illness onset […] Maximum virus excretion from the respiratory tract occurs on about day 10 of illness and then declines.
Which is the transposition or converse compared to the charts for nCov-19 infection in the first section (repeated below) wherein the maximum virus load is in the nose (for maximum,earlyaerosol transmissibility!) in the first few days after onset and then as nasal load declines towards the end of the first week, the load in the throat increased, and then both declining into the second week:
SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients
Note the above charts presumably aren’t as statistically significant as the data above compiled for the entire SARS epidemic. Yet combined with the significant other evidence I cited in the previous section, I’ll take it to be likely representative or proximate to the statistically significant reality.
Expected Timeline
I warned about a pandemic at the end of my December 16, 2019 blog. Research so far indicates the initial surge in human-to-human transmission in Wuhan began in mid-December, but first public news was December 31.
The “don’t test, don’t tell” policy is congruent with what the “Allied Powers” did to cover-up the 1918 Spanish flu and ostensibly Trump has been trying to make it to end of flu season (warmer, less humid weather) without a panic hoping to avoid economic recession during his (“it’s the economy, stupid”) reelection campaign. Officials know damn well that if they test all with symptoms and/or do probabilistic serology sampling that it will likely show 1000s, 10,000s or perhaps up to 100,000s of Americans already infected.
Presuming the actual death rate (when all infected are accounted for) will be much lower, perhaps even less than 1%, then unlikely to have more than 10,000 deaths in the USA before end of the current flu season which typically peaks February–March, and tapers off in April. Being novel nCov-19 might not tail off entirely in summer though:
Next flu season after the November presidential election is when I have been expecting millions to be infected in the USA and confirmation via random serology sampling. And per Armstrong’s model which in 2016 predicted this pandemic, 2021/22 flu season is likely to be the peak with perhaps up to 40–80% of the population infected.
Whether the case fatality rate (CFR) will remain low upon reinfections and vaccines remains to be seen, but that could be an ongoing dysfunctional immunopathology (think HIV → AIDS timeline) phenomenon perhaps over another 13 years (per Armstrong’s model)?
@Strelnikov wrote:
Freakiest aspect to me is the spread of this disease tracks very closely to the spread o the Zombie disease in the novel “World War Z”. In the novel, the outbreak was local to an area in China and concealed by their government until the diaspora had spread it world wide.
It is of utter importance that people understand the problem with dead or attenuated vaccines for SARS virii. In ever trial so far, such vaccines have made infection with SARS virii much worse.
This is an excellent post full of factual information regarding the current pandemic and virus involved. I very much appreciate your posting it.
Thanks!
It also attacks the nervous system.
https://doi.org/10.1002/jmv.25728
"Increasing evidence shows that coronavriruses are not always confined to the respiratory tract and that they may also invade the central nervous system inducing neurological diseases. The infection of SARS‐CoV has been reported in the brains from both patients and experimental animals, where the brainstem was heavily infected. Furthermore, some coronaviruses have been demonstrated able to spread via a synapse‐connected route to the medullary cardiorespiratory center from the mechano‐ and chemoreceptors in the lung and lower respiratory airways. In light of the high similarity between SARS‐CoV and SARS‐CoV2, it is quite likely that the potential invasion of SARS‐CoV2 is partially responsible for the acute respiratory failure of COVID‐19 patients. Awareness of this will have important guiding significance for the prevention and treatment of the SARS‐CoV‐2‐induced respiratory failure."