Blood Urea Nitrogen : Creatinine (BUN:Cr) and Azotemia
Blood Urea Nitrogen (BUN) is the metabolic end product of amino acids, pyrimidine and ammonia metabolism. Excretion in urine is the major way to get rid of BUN from the body. After being filtered in the glomerulus, a little is reabsorbed by the PCT cells. The rest will be excreted in the urine. If the glomerular filtration rate (GFR) is decreased, more urea can be reabsorbed by the PCT cells because they have more time to reabsorb as the fluid is flowing slowly. Similarly, if the GFR increases less can be reabsorbed.
BUN can also be lost from the body via skin or bowel, but only when the concentration on BUN in plasma is extremely high.
Factors that affect the serum level of BUN includes GFR, Proximal tubule reabsorption, Protein content in the diet and Functional status of the urea cycle.
Creatinine is the metabolic end product of creatine in muscles. Creatinine is filtered in the glomerulus and excreted along with urine. After filtration none of the creatinine is reabsorbed back. All goes down the toilet!!
With muscle wasting, serum creatinine levels will go down.
Any condition that decreases filtration at the glomerulus or obstructs free flow of fluid in the nephrons will increase serum levels levels of both BUN and Creatinine. This is known as Azotemia.
But the proportion of increase of these two substances most of the time will not be the same. Thus the normal ratio of serum BUN and serum creatinine (BUN:Cr) will be altered in most cases of azotemia. Normal Serum BUN:Cr is 15.
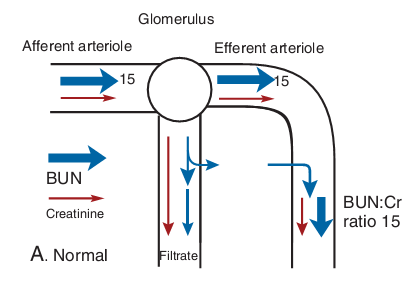
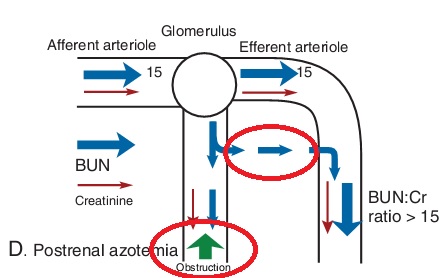
image from Goljan Rapid Review Pathology, 4th edition
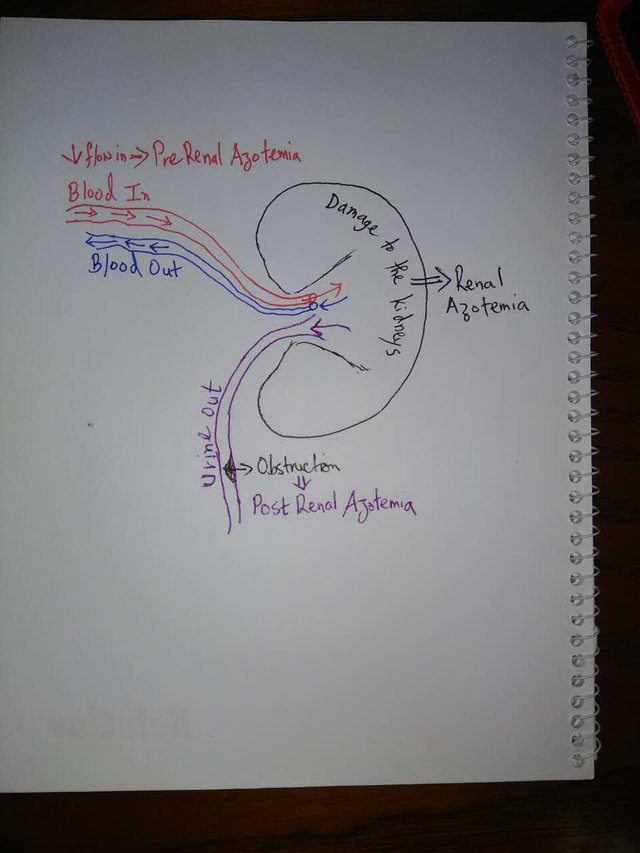
Based on the causes, Azotemia can be broadly divided into :
- Pre-Renal Azotemia
- Renal Azotemia
- Post-Renal Azotemia
Before I go into detail how each of these different Azotemias alter the BUN:Cr, let's look at a very basic schematic :
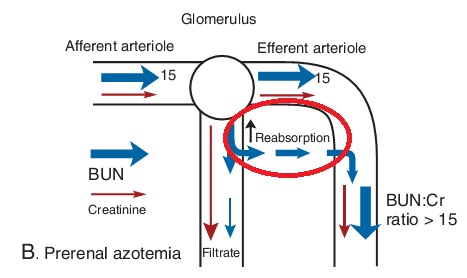
PRE-RENAL AZOTEMIA
As we see in the schematic above, pre-renal azotemia is caused by a decrease in blood flow into the kidneys. Most often this is due to decreased cardiac output caused by conditions like congestive heart failure and circulatory shock, or conditions like renal artery stenosis which also decreases inflow of blood into the kidneys.
Decreased flow into the kidney decreases GFR. This causes both BUN and creatinine to back up in the blood and levels increase (azotemia). But this doesn't alter the BUN:Cr ratio because both BUN and creatinine levels rise proportionately due to the decreased GFR.
But what changes the ratio is the fact that, as GFR decreases, the PCT cells have more time to reabsorb BUN from the filtrate. This causes a proportionate increase in the level of BUN in the blood compared to creatinine (all the filtered creatinine will be excreted).
Now it's just simple mathematics!! Both BUN and Creatinine levels increase in blood. But level of BUN increases more. Thus the BUN:Cr will be higher than normal, i.e. >15.
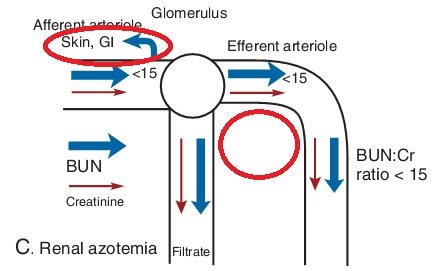
RENAL AZOTEMIA
When there is increased levels of BUN and creatinine in blood due to damage to the kidneys, we call it Renal Azotemia. Conditions like acute tubular necrosis, acute glomerulonephritis, chronic renal failure, etc. can significantly damage the kidney parenchyma and cause Renal Azotemia.
The damage to the kidney parenchyma will naturally decrease GFR (because the glomerulus is part of the kidney parenchyma, duh!!) and proportionately increase BUN and Creatinine levels. This decrease in GFR is much more than the decrease we've discussed in Pre-Renal Azotemia. Thus there will be a much higher increase of both BUN and Creatinine in the blood. Now recall that "BUN can also be lost from the body via skin or bowel, but only when the concentration on BUN in plasma is extremely high." In renal azotemia, we usually have such extremely high levels of BUN.
Now let's do some simple mathematics again!! Both BUN and creatinine levels increase proportionately in the blood. But some of the BUN is being lost via skin, GIT, etc. What happens to the BUN:Cr ratio? After the loss of BUN from skin and GIT, we have proportionately higher levels of creatinine. Thus the BUN:Cr ratio is now lower than normal.
Furthermore, in renal parenchyma damage, the PCT cells are also damaged and are not functioning properly. So even though the GFR is decreased (and there should be an increased reabsorption of BUN from the filtrate), there is NO REABSORPTION of BUN from the filtrate. So both BUN and creatinine are being lost which further decreases the proportionate levels of BUN in the blood (note that this isn't having any effect on the proportionate levels of creatinine because creatinine was not being reabsorbed normally anyways). Thus the BUN:Cr ratio falls further below 15.
POST-RENAL AZOTEMIA
Post-Renal Azotemia results from obstruction to the outflow of urine past the kidneys, i.e. the ureters or the urethra. Usually if only one of the ureters is obstructed and the other one is working fine, we probably won't see post-renal azotemia because the unobstructed kidney is more than capable of compensating 100% for the obstructed kidney (which is why we can live a completely healthy life with only one healthy kidney).
But if there is bilateral obstruction of the ureters, or an obstruction in the urethra, post-renal azotemia will develop.
Conditions that can cause these obstruction include benign prostatic hyperplasia, blockage by stones, blockage due to cancer or external compression.
This obstruction decreases urine outflow from kidney and the pressure backs up all the way to the glomerulus, obstructing filtration, thus GFR is decreased. It's like when you obstruct one end of a water pipe, the pressure backs up all the way to the starting of the pipe and water flow through the whole pipe decrease behind the obstruction.
This decrease in GFR is not as severe as in renal azotemia, but more similar to pre-renal azotemia. Thus we initially have a situation very similar to what happened in pre-renal azotemia. Both BUN and Creatinine backs up in blood in proportionate amounts. But the decreased GFR allows more time to the PCT cells to reabsorb more BUN and eventually we end up with a BUN:Cr >15.
At this point, it isn't really possible to differentiate between pre - and post-renal azotemia just by the BUN:Cr ratio. We have to take into account the signs and symptoms the patient presents with to make our diagnosis. For example, Decreased blood pressure in situations of decreased cardiac output and pain depending on the location of obstruction in the urinary tract (check out the post on urinary tract stones for more information : https://steemit.com/science/@simplifylife/urinary-stones-understanding-the-basics).
Initially there is no damage to the parenchyma of the kidney. ut if the obstruction is not treated and it persis for a long period of time, the pressure build up will damage the kidney parenchyma (in a very similar way as a water pipe would burst if you obstruct it long enough to create very high pressures within). Once the kidney parenchyma is destructed, we'll have the situation similar to renal azotemia and the ratio of BUN:Cr will be less than 15.
Sources :
Goljan Rapid Review Pathology, 4th edition
Alright guys, that's it for now!! Hope you learned something today!!
Start Upvoting to increase your Curation Rewards. Resteem this post and maybe more people out there might find this useful.
If you enjoy medical topics, health tips, or steemit tutorials for beginners and newbies, please make sure to follow me at @simplifylife
Peace!!
Good post. I suggest you use a spell checker next time and proof read it once or twice. ;)
Thank you very much. I am trying to do the proof reading, but every time it seems I'm missing some words lol!! Will keep trying till it gets perfect!!
Thanks for sharing :-) @simplifylife I am following. Best of Luck !
This post received a 1.6% upvote from @randowhale thanks to @simplifylife! To learn more, check out @randowhale 101 - Everything You Need to Know!
This post recieved an upvote from minnowpond. If you would like to recieve upvotes from minnowpond on all your posts, simply FOLLOW @minnowpond
This post has received a 2.70 % upvote from @buildawhale thanks to: @simplifylife. Send at least 0.50 SBD to @buildawhale with a post link in the memo field for a portion of the next vote.
To support our curation initiative, please vote on my owner, @themarkymark, as a Steem Witness