Beware ... Your mother or grandmother may be sick with osteoporosis!!!
Hi steemians.
What is osteoporosis?
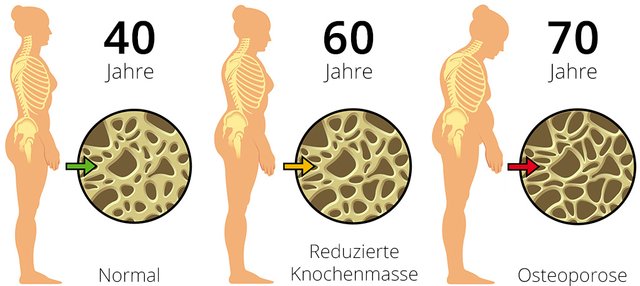
Diffuse skeletal disease characterized by a decrease in bone mass and an alteration of bone micro-architecture that increase bone fragility and the risk of fractures.
Osteoporosis or "fragile bone disease" today represents a real public health problem. While postmenopausal women appear particularly affected, sex hormone deficiency is not the only risk factor.
Osteoporosis has long been thought to be an exclusively female disease. Although men are also affected, it is known that estrogen deficiency (female sex hormones) promotes bone loss. This influence is particularly visible when menopause occurs early (before age 45) or following surgery. In the same way, late puberty may be a risk factor.
Risk factors
Extensive epidemiological studies have uncovered several risk factors:
1. Age and sex:
The occurrence of osteoporosis is primarily related to sex and age. If one in eight men is touched after age 50, at that age one in three women suffers. This proportion increases with the years since one woman out of two is concerned after 75 years.
First explanation: the lengthening of life expectancy. This makes it possible to assert that, in the coming years, there will be a true "epidemic of osteoporosis", in the words of Gro Brundtland, the Director General of WHO.
Women are particularly affected because of decreased estrogen secretion at menopause. During the first 5 years after menstruation, it is estimated that women lose 5 to 15% bone density, then 2% per year thereafter. Other gynecological factors may be retained: late puberty, early menopause by oophorectomy or natural (that is, before age 45), or prolonged amenorrhea.
2. Genetic factors:
Although it is difficult to ensure in the current state of knowledge that there is a "pure" genetic factor, the bone capital of a person is often determined by heredity. The lighter its bone structure, the more likely it is to develop osteoporosis. A family history of fractures is one of the hints a doctor looks for with a hint of osteoporosis.
Recently, a family predisposition has been identified 1. Brothers and sisters of people with osteoporosis are six times more likely to have low bone density than the general population.
This is the result of a study conducted by Dr. Duncan on 170 families. The English researchers have also identified 8 genes potentially responsible for this disease.
3. Too little weight:
Excessive thinness is a risk factor. The fatty tissue is indeed able to produce estrogen (female hormones).
4. Ethnic origin :
Caucasian subjects (European and Asian) have the lowest bone density. That of black-skinned individuals is stronger.
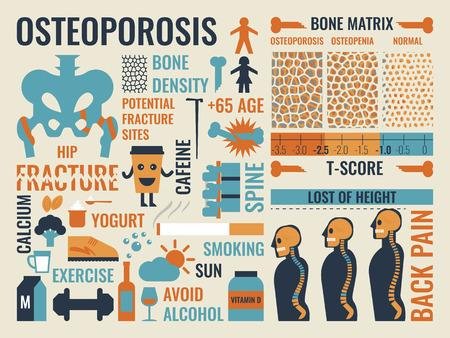
5. Food factors:
More than three cups a day of caffeine and more than two glasses of alcohol are all penalizing factors. Similarly, physical inactivity is also detrimental. In contrast, vitamin D and calcium intake is to be favored in the diet or by exposing oneself reasonably to the sun.
6. Environmental factors:
Smoking and being too sedentary have also been identified as contributing to the weakening of your bone stock.
7. Associated diseases:
Prolonged or excessive use of certain corticosteroid-based treatments, and certain diseases (hyperthyroidism or diabetes) interfere with calcium and may lead to so-called "secondary" osteoporosis as induced by other diseases or therapies.
A large study conducted by scientists from the National Institute of Mental Health on more than 7,000 women identified a greater risk of osteoporosis in women with major depression. The mechanism involved is not yet identified, but high blood cortisol levels, often found in depressed patients, could cause bone loss.
What are the consequences of osteoporosis?
The complication of osteoporosis is fracture. The most common are vertebral fractures, femoral neck fractures or forearm bones, but almost all bones can be fractured due to their fragility (except skull, fingers, toes). and the cervical spine).
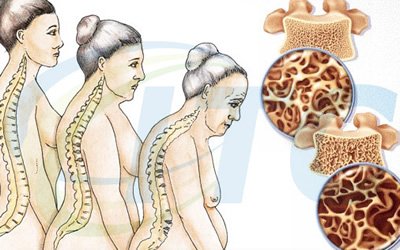
1. The occurrence of multiple vertebral fractures:
leads to a reduction in size more or less important (sometimes responsible for compression of the abdomen, oesophageal reflux [burning sensation in the esophagus], shortness of breath, etc.. ), deformations of the column (arching back, modification of the curvatures of the spine, pain of the lower back and sometimes pain of contact between the ribs and the pelvis due to the loss of size) and a repercussion on the quality of life. Lower back pain is often aggravated by effort, exercise, standing or sitting for long periods of time and is relieved by rest.
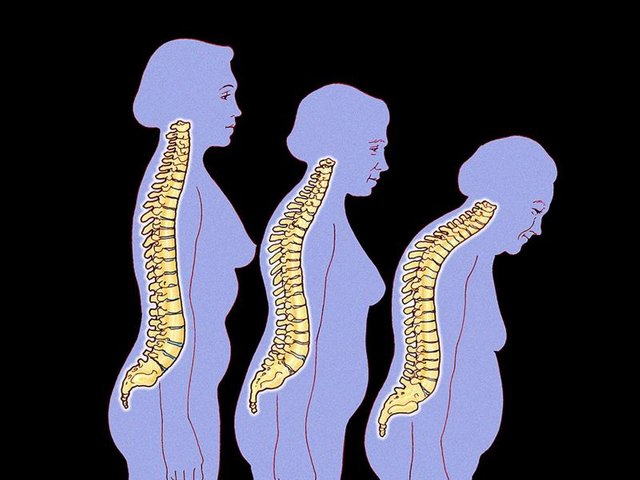
Image source Reduction in size.
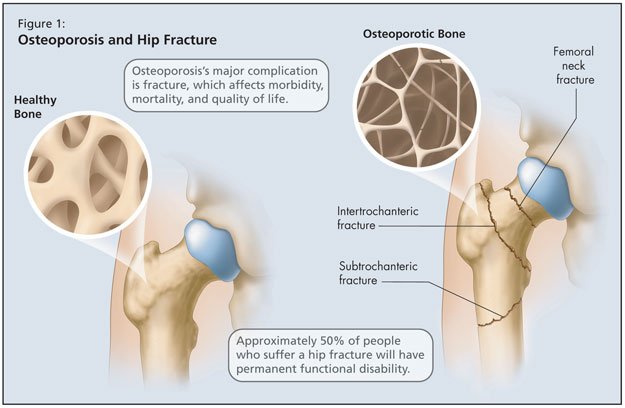
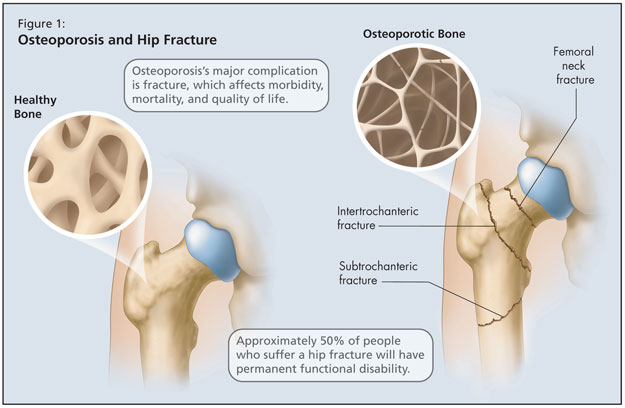
2. The fracture of the femoral neck:
It is serious because of the risks of general postoperative complications related to the intervention (phlebitis, embolisms, infections and other complications related to the bed rest). It sometimes requires the establishment of a prosthesis which itself can be complicated (infection, dislocation, wear, etc.). Returning home after an intervention in such a context is not always possible. We often notice in the suites an important fear of falling again; there is a risk of dependence. After a hip fracture, 80% of patients experience a loss of autonomy, 40% require assistance to walk, 30% have a long-term disability and 50% do not regain their independence after one year.
3. Repercussions in everyday life:
A fracture episode often leads to a reduction in activity, functional abilities, gait and postural disorders (retropulsion, standing phobia, oppositional hypertonia), thus increasing the risk of relapse. After a wrist fracture, for example, discomfort in everyday life can persist beyond six months, including difficulty in handling objects, cooking, washing or clothing.
This is why, after a fracture, there is often a placement in a retirement home.
How to prevent osteoporosis?
1. Lifestyle
Regular physical activity (sport in charge)
Eviction of risk factors (tobacco, alcohol, coffee, tea)
Balanced diet.
Sufficient calcium ration (1g / d).
Correction or prevention of vitamin D insufficiency.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
2. Correction of risk factors for falling
Develop the home,
Reduce the dosage of sleeping pills.
Detect and treat an orthostatic hypotension and visual disturbances.
Treatment of walking disorders.
Treatments of osteoporosis
Five types of treatments are currently available to reduce the risk of fractures. They act either by decreasing bone resorption (SERM, bisphosphonates, Denosumab), or by stimulating bone formation (teriparatide). A single treatment (strontium ranelate) stimulates bone formation while decreasing resorption.
1. SERMs (Evista®, Optruma® ...)
Also inhibit bone resorption. They act like estrogens on bone tissue but, unlike estrogen, do not have a stimulating effect on the uterus or the breast. These molecules, which are not hormones, are capable, according to the tissues, of inducing via the estrogen receptors, pro or anti-estrogenic effects. These molecules have a protective role against osteoporosis, without increasing, or even decreasing the risk of cancer of the uterus or breast.
2. BIPHOSPHONATES (FOSAMAX®, ACTONEL® ...)
Bisphosphonates are not hormones. These drugs mainly inhibit bone resorption and, more generally, the process of bone remodeling. They have the property of fixing themselves exclusively in the bone to prevent its destruction. They can bind themselves securely to the bones and eventually integrate into the skeleton. They stop bone loss by preventing osteoclasts from destroying the tissue on the surface of the bones.
3. STRONTIUM RANELATE (PROTELOS®)
Strontium ranelate is characterized by an original mode of action, which allows it to play on both fronts: increase bone formation and limit resorption. Tested on nearly 7,000 people in two studies, this compound significantly reduces the risk of recurrent vertebral fractures, new fractures and, to a lesser extent, non-vertebral fractures. The summary of the characteristics of the product mentions disorders of the nervous or gastrointestinal system but in 2007, the Afssaps added that this drug could lead to a syndrome of hypersensitivity drug or syndrome Dress, a serious allergy which can reach the liver , kidneys and lungs. The drug agency had indicated that the occurrence of a rash, regardless of the age of treatment, should lead to discontinuation of treatment and to consult a doctor. In September 2011, this drug is at the heart of a controversy. According to the newspaper Libération, a report from the European Medicines Agency (EMEA) accuses the laboratory Servier for hiding health authorities cases of side effects of Protelos. Charges denied by the laboratory Servier. Afssaps is currently reassessing the benefit-risk of this drug.
4. PARATHORMONE (PTH) 1-34 OR TERIPARATIDE (FORSTEO®)
Parathyroid hormone or parathyroid hormone is secreted by the parathyroid glands. It controls the metabolism of calcium and phosphate in the body. Administered as a daily injection, parathyroid hormone strongly stimulates bone formation. This drug, reimbursed only in women with at least two vertebral fractures, is reserved for severe forms and can not be prescribed for more than 24 months.
5. THE DENOSUMAB (PROLIA®)
Denosumab (Prolia®) is a monoclonal antibody that inhibits the formation, function and survival of osteoclasts, cells responsible for bone resorption. This effect is achieved by specifically inhibiting an essential substance (mediator) of bone resorption: the ligand RANK. Available since October 2013, denosumab is indicated for the treatment of postmenopausal osteoporosis to reduce the risk of vertebral, non-vertebral and hip fracture in patients at high risk of fracture. This drug is administered as a subcutaneous injection every 6 months but should only be used as a 2nd line, that is, in patients who have been previously treated with bisphosphonates.
Source:
- GRIO (Research and Information Group on Osteoporosis)
- "Strontium ranelate, a new therapeutic agent in postmenopausal osteoporosis", Pierre J. Meunier, Medicine Sciences, Volume 20, N ° 6-7, June-July 2004
- High Health Authority (HAS). Good use of the drug - The drugs of osteoporosis, June 2014.
Follow Me @sparganose
There are ways to improve bone density that don’t involve medication.
People just accept that they are getting older and the bones become more frail, but they don’t have to.
There is a safe and easy way to reverse the decline of bone density. Called osteogenic loading, just a few minutes a week can cause bone density to GROW! It is short resistance exercises easy for kids and grownups alike.
When half of Caucasian women over 50 have osteoporosis, osteo loading is the way to go. In six months, instead of declines, studies show an increase of 8% in bone density when doing osteo loading — 4x more than traditional weight bearing activity!
Nice idea thank you for sharing it. actualy with with all the side effects of the drugs this work can be a good alternative
This post has received a 0.67 % upvote from @buildawhale thanks to: @sparganose. Send at least 1 SBD to @buildawhale with a post link in the memo field for a portion of the next vote.
To support our daily curation initiative, please vote on my owner, @themarkymark, as a Steem Witness
Resteemed by @resteembot! Good Luck!
Curious?
The @resteembot's introduction post
The @reblogger's introduction post
Get more from @resteembot with the #resteembotsentme initiative
Check out the great posts I already resteemed.