Pharmacology #2 : Salt + Water = Hypertension
Hey guys, this is the 2nd series of my Pharmacological content. I love Pharmacology and that’s why I would love to share things that I have understood. This time I’ll be discussing about a much commoner problem in our modern world, Hypertension. I bet everyone that’s reading this has a family member or two with Hypertension, or at the very least heard about it before. I’m going to discuss about the ways to combat Hypertension via medications. As usual, in order to treat a disease, you need to know about the disease. In this case, I’ll explain about how our body tries to maintain blood pressure towards its normal level, which is 120/80mmHg.
Based on the hydraulic equation, arterial blood pressure which is taken as BP is directly proportionate to the product of blood flow (CO = Cardiac Output) and the resistance through the arteries or peripheral vascular resistance (PVR).
BP= CO x PVR

Autonomic Nervous System:
This system is the first one to provide response when there’s changes in the blood pressure. Before we proceed to examples of related scenarios, let’s understand the concept of Alpha and Beta receptors briefly. Alpha receptors are widely expressed the blood vessels, and their activation leads to blood vessel constrictions, both artery and vein.
- Alpha 1 receptors are located mostly in the vascular smooth muscles, pupillary dilator muscles, prostate, and the heart.
- Alpha 2 receptors are situated mainly in the platelets, some vascular smooth muscles and fat cells.
- Beta 1 receptors are embedded in the heart and juxtaglomerular cells. It increases the heart rate and renin release respectively.
- Beta 2 receptors are slightly different. As they are mainly found in the respiratory, uterine and vascular smooth muscles, they promote relaxations, instead of constriction which is the opposite of alpha receptors.
Agonists in simple terms, are the good guy. They are the supporters. Antagonists as the name implies, are the bad guys. They do not support the activation of the receptors. These terms are important later as they are pretty much going to be repeatedly use in the pharmacological section of this blog.
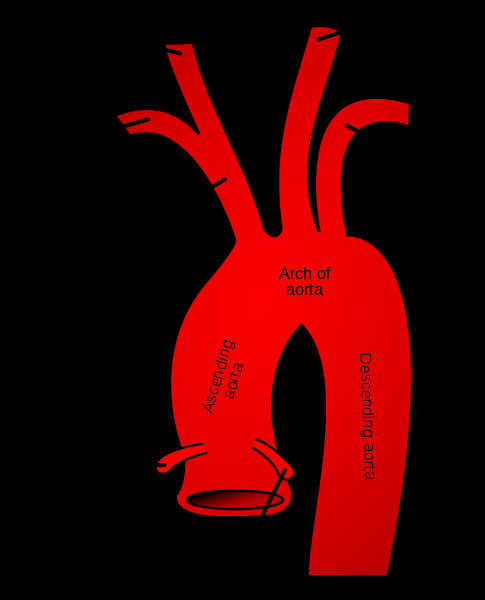
An example of situation is when we quickly stand up from a sitting or lying position. Our body is blessed with baroreceptors and chemoreceptors. Baroreceptors are located in the carotid sinus and the aortic arch. They act as sensors and sensitive to any changes in the blood pressure. Usually they are stimulated when the blood vessels are stretched out. So in this case, when our blood pressure starts to drop when we began rise from sitting, the baroreceptors send signals to the Nucleus of the Tractus Solitarius in the brain, and stimulate the vasomotor center. The vasomotor center provides signals to the peripheral arterioles throughout our body as well as the heart via nerves. It’s like a chain of reaction and it happens very rapidly.
The peripheral arterioles will then constrict to increase the peripheral vascular resistant. Remember BP= CO x PVR ?
Yes, when PVR increases, BP will increase too. That’s not all. Since the heart receives impulse as well, the heart will beat faster to increase the cardiac output which further improves the blood pressure.
So the next question would be.. why does this happen ?
Okay. Imagine what happens when you quickly stand up? Your blood will pool on your lower half of your body due to gravity pull. Fewer blood will return to the brain because of this. The brain is one of the main organ that our body will try its best to protect. Hence, this reflex is important to keep the brain alive. Other similar situations include when there is a reduction of intravascular volume such as in bleeding or loss of salt and water via the kidneys.
Renin-Angiotensin-Aldosterone System
This system involves in the long term blood pressure control which is the opposite in the previous system. As the name implies, RAAS involves Renin, Angiotensin, and Aldosterone. Let’s go to each component of RAAS.
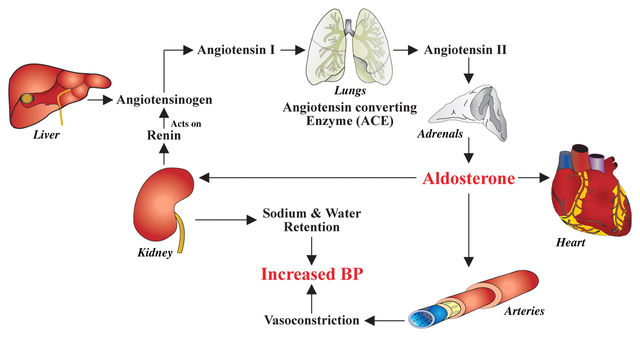
Renin is an aspartyl protease enzyme that originates from the kidney. Within the kidneys, renin is synthesized, stored, and release in the juxtaglomerular cells. Similar to the autonomic nervous system, the kidneys have their own baroreceptors to detect any blood pressure changes. When it is stimulated, renin is then released to the blood stream.
So what does the renin do?
Renin catalyzes the conversion of Angiotensinogen to Angiotensin. Try to remember all these terms at it is related to the drugs used to combat hypertension. Angiotensinogen comes from the liver. The production of this protein is increased by the actions of corticosteroids, estrogens, thyroid hormones and angiotensin II.
Angiotensin I is the product when renin cleaves the angiotensinogen. Angiotensin I has little biological activity. So let’s just recap a little bit, Angiotensin is converted to Angiotensin I via Renin. Alright.
So how does Angiotensin I becomes Angiotensin II?
That’s where ACE kicks in. ACE is the shortform of Angiotensin Converting Enzyme. It is actually a dipeptidyl carboxypeptidase enzyme that cleaves Angiotensin I to Angiotensin II. Angiotensin II is one of the main protein that regulates our blood pressure. It has four actions
- Vessel contractions – Angiotensin II is very potent pressor agent that causes direct contraction to the arteriolar smooth muscles.
- Adrenal Cortex and Kidneys – It acts directly on the zona glomerulosa of the adrenal cortex to stimulate Aldosterone release, increase proximal tubular sodium reabsorption and inhibits renin release.
- Brain – It stimulates drinking, increase the secretion of antidiuretic hormone (a hormone that inhibits urination), as well as Adenocorticotropic Hormone (ACTH). ACTH too stimulates the release of Aldosterone.
The last component of the RAAS is the Aldosterone. Aldosterone is known as mineralocorticoid and is synthesized mainly in the zona glomerulosa of the adrenal cortex, as I mention above. The production of this hormone mainly depends on Angiotensin II and the ACTH. Without ACTH, Aldosterone level would fall into half of its usual amount in the blood.
How does Aldosterone works?
It promotes the reabsorption of sodium from the distal part of the distal convoluted tubule, collecting ducts of the kidneys, sweat, salivary glands and even the gastrointestinal mucosa. It basically helps our body to retain salt, which then retains water. Both of these elements contributes to the increase of blood pressure. Increase in water causes the increase in Cardiac Output. Hence, CO increase leads to BP increase. Just remember the equation!!
After understanding the basic concepts of blood pressure regulation, let’s look at the treatment options. The mechanism of action of the drugs used in treating high blood pressure is targeted to the specific parts of the Autonomic Nervous System, RAAS and Water-Sodium balance which results in the reduction of blood pressure level of an individual.

Autonomic Nervous System related drugs
- Centrally Acting
- Alpha Blocker
- Beta Blocker
- Vasodilators
- Calcium Channel Blockers
Centrally Acting drugs, or also known as Centrally Acting Sympathoplegic Drugs:
These drugs were once used widely in the treatment of hypertension. They act by reducing sympathetic outflows from vasomotor centers in the brainstem. Based on what I have explained before, the sympathetic outflows passes the signal to all peripheral arterioles in the body, causing generalize vasoconstriction, leading to increase in BP. Since the signaling pathway is blocked, they causes the reduction in blood pressure level.
Examples of drugs are Methyldopa and Clonidine.
Methyldopa is now primarily used only in Pregnancy Induced Hypertension due to its high safety profile. Most anti-hypertensive drugs are contraindicated in Pregnancy as they might exhibit teratogenic effects which could harm the fetus. Clonidine reduced the heart rate and causes the relaxation of blood vessels, leading to the lowering of blood pressure.
Alpha Blockers
These drugs as the name implies, blocks the alpha receptors which is mostly located in the vascular smooth muscles. This leads to the relaxation of smooth muscles, and then lowers the blood pressure. These drugs acts on both resistance and capacitance blood vessels, leading to more reduction in blood pressure in the upright than in the lying position. Hence it might worsen postural hypotension. Since it exhibits its some effects on the prostate, it is quite useful in hypertensive men with enlarged prostate in cases such as benign prostate hyperplasia.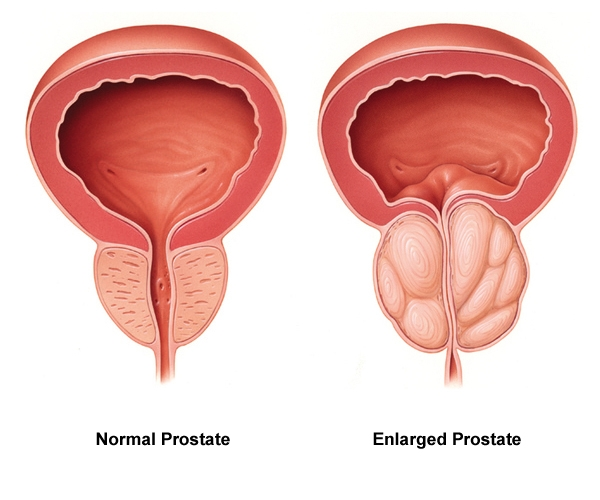
Examples of drugs are Prazosin, Terazosin and Doxazosin
Beta Blockers
Their way of reducing blood pressure is via the blockade of B receptors in the heart. Heart will pump slower, causing reduced CO, leading to lower BP. Moreover, B blockers inhibits reflex tachycardia which is often induced by vasodilators.
How does it happen?
Alright. When a vasodilating agent or an alpha blocker, the blood vessels dilate. Our baroreceptors will then detect the situation and stimulates the heart via the sympathetic pathways to pump faster (tachycardia). This is another example of how our body responds when our blood pressure drops. B Blockers block this reflex, making the drugs more potent in lowering the individual’s blood pressure. As I mentioned earlier, B receptors are located in few other places apart from the heart, such as the lungs. Hence, a selective B blocker is preferred than a non-selective one.
Example of non-selective B-Blockers: Propanolol, Labetolol, Carvedilol
Example of selective B-Blockers: Metoprolol, Atenolol
Propanolol was the first Beta Blocker to be effective in reducing blood pressure.
So why a non-selective B-Blocker such as propranolol does is widely replaced by selective agents?
It is because Propranolol affects the other Beta receptors, including those in the lungs. Stimulation of Beta 2 receptors in the lungs will result in relaxation of bronchial smooth muscles. In a normal human, the blockade of this receptor probably won’t do anything. However, in cases like patients with asthma, the consequences could be severe as the bronchial smooth muscles are not in relaxed state. In individual with asthma, their bronchial smooth muscles are constantly constricted which results in difficulty in breathing. Hence, propranolol is contraindicated in asthmatic patients. Propranolol could mask symptoms of hypoglycemia in Diabetic patients. Symptoms of hypoglycemia (or sugar hunger) are tachycardia, tremor, and feeling anxious. Propranolol hides all these symptoms, causing the individual to be unaware of having hypoglycaemia. Labetolol is mainly used in pregnancy, similar to methyldopa. Both drugs are proven to be safe to the fetus. Metoprolol and Atenolol are cardioselective and people are using it more often now to treat hypertension.
Vasodilators
They have many mechanisms which are not related to those I have mentioned above but they do dilate the blood vessels. Drugs such as Nitroprusside and Hydralazine release nitric oxide. Nitric Oxide is a potent vasodilator. Minoxidil and Diazoxide reduces blood pressure via the opening of potassium channels, which causes hyperpolarization. Hyperpolarized smooth muscles do not constrict, thus causing vasodilation. These drugs work perfectly in combination with other antihypertensive agents that opposes the reflex tachycardia which I have mentioned before.
Calcium Channel Blockers

This class of drug has many other medical benefits including antianginal and anti-arrhythmic effects. They inhibit calcium influx into the arterial smooth muscle cells which results in vasodilation. Calcium influx plays a part in vasoconstriction. There are two types of calcium channel blockers: Dihydropyridine and Non-Dihydropyridine.
Examples of Dihydropyridine CCB: Amlodipine, Felodipine and Nifedipine
Examples of Non-Dihydropyridine CCB: Verapamil and Diltiazem.
I’m sure some of you heard the names of one of these drugs before. Amlodipine is quite a famous drug that doctors usually prescribe for hypertension.
Let’s move on to agents those affecting the RAA system. You guys can refer back to the Renin-Angiotensin-Aldosterone System which I have explained earlier.
RAAS related drugs:
- Renin Inhibitor
- Angiotensin Converting Enzyme Inhibitor or ACE Inhibitors
- Angiotensin Receptor-Blocking Agents
As the name implies, Aliskiren inhibits renin production which results in the inhibition of Angiotensinogen to Angiotensin I conversion. ACE inhibitors are frequently prescribed too.
Examples are Captopril, Enalapril, and Perindopril.
They inhibit the angiotensin converting enzyme which halts the conversion of Angiotensin I to Angiotensin II. ACE inhibitors have a useful role in treating individuals with chronic kidney disease as they stabilized renal function. They are often prescribed to Diabetic individuals as these individuals are prone to get Diabetic Nephropathy, which later often develops to Chronic Kidney Disease. One of the commonest side effect of ACE inhibitors is dry cough.
Angiotensin Receptor Blockers or ARBs such as Telmisartan, Losartan, and Valsartan are agents that block angiotensin receptors which are in the blood vessels, kidneys, and brain which I have mentioned earlier. They inhibit vasoconstriction as well as Aldosterone release.
Drugs that alters Sodium and Water Balance or Diuretics.

If you still remember the famous equation, BP = CO x TPR? Water and Sodium level affects the Cardiac Output. Higher water volume in the blood vessels will result in more blood that the heart needs to pump. Diuretics promote water loss through urination and results in lower blood pressure.
Examples of diuretics:
- Thazide such as Hydrochlorothiazide
- Loop diuretics such as Furosemide
- Potassium sparing diuretics such as Spironolactone
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
So now, how do we choose which drugs to use?
Let the doctors decide hahahaha. I’ll provide a general guideline here.
- Mild hypertension: Thiazides, CCBs, ACE inhibitors, ARBs.
- Hypertension with heart failure: Thiazides, Loop diuretics, B Blockers, ACE inhibitors, ARBs
- Hypertension with Benign Prostatic Hyperplasia: Alpha Blockers
- Hypertension with Arrhythmias: Verapamil, Diltiazem
- Hypertension with Angina: CB
- Hypertension with Gout: ARBs
- Severe Hypertension: Loop Diuretics, and other Antihypertensives
- Pregnancy Induced Hypertension: Methyldopa, Labetolol
- Hypertensive Emergencies: Vasodilators, and Labetolol (in pregnancy)
That’s a lot to take in huh? Haha. To be a doctor is not easy because someone’s life is at stake. Good choices should be made for the patient’s benefits. Some quick facts about hypertension taken from CDC.
{kind=link}
- About 7 of every 10 people having their first heart attack are hypertensive
- About 8 of every 10 people having their first stroke are hypertensive
- About 7 of every 10 people with chronic heart failure are hypertensive
- Hypertension is the cause of 12.8% of total deaths
So, that’s about it. In short, we should take care of ourselves and the very first step is to modify our lifestyle. Eat healthier meals, exercise regularly and avoid excessive salt intake! As the saying goes, you can’t enjoy wealth if you aren’t in a good health. Have a good day :)

References
- Katzung et al. Basic & Clinical Pharmacology .Singapore: McGrawHill, 2012. Print
- Effects of High Blood Pressure. Centers of Disease Control and Prevention. Retrieved on April 5, 2018, from https://www.cdc.gov/bloodpressure/effects.htm
- Raised Blood Pressure, Global Health Observatory Data. WHO. Retrieved on April 5, 2018, from http://www.who.int/gho/ncd/risk_factors/blood_pressure_prevalence_text/en/
- World Hypertension Day 2017: Know your numbers. Pan American Health Organization. Retrieved on April 5, 2018, from http://www.paho.org/hq/index.php?option=com_content&view=article&id=13257%3Adia-mundial-de-la-hipertension-2017-conoce-tus-numeros&catid=9283%3Aworld-hypertension-day&Itemid=42345&lang=en
- Pathophysiology of Hypertension. Wikipedia. Retrieved on April 5, 2018, from https://en.wikipedia.org/wiki/Pathophysiology_of_hypertension
I found the last 4 points about hypertension's relation to stroke and heart conditions, to be quite interesting. I tended to think of hypertension as much more benign than all that.
Is salt and water the only substances that influence blood pressure, or are there other minerals that interplay with these two, like magnesium or whatnot?
Great post. Discussed with my wife who has HOCM and needs to minimize salt intake.
Hello,
The initial post above should be taken as a good primer, but in no way should it supplant the information given to you by your physician, as HTN management is far more complex and is often tailored to the individual patient (as a practicing physician myself)
With HOCM, minimizing sodium intake can help, but the main issue is the outflow tract obstruction which occurs due to increased intraventricular septal mass. The drug of choice, or rather the therapeutic effect of choice with this particular condition is a reduction of heart rate, not necessarily effective circulating volume. With a reduced heart rate, which is often achieved with Beta Blockers like metoprolol, there is increased ventricular filling time, and an improved cardiac output. With fast heart rates (often HR above 90) there is an effective outflow tract obstruction due to the asymmetric interventricular septum which causes decreased cardiac output and an unsafe drop in blood pressure.
Thank you for the information. She has been stable on nadolol and some others. I know limitation of Na intake is recommended for healthy people in general.
Thanks for the great input doc !!
This is very detailed. Well done.
Thank you @vanessahampton :)
Hello and welcome to steemit!
I had been looking for a practical article on hypertension and treatments for a while now. They are either too complicated for non-medical professionals or way too simplified. So thank you for your input. I have a question: have you noticed a correlation between deficiency of vitamins B12/ D and hypertension?
I tried my best to balance out the article from being too complicated or too simple. From what I understand, Vitamin B12 is an important element for hematopoiesis, or blood formation. Lacking this vitamin can result in a type of anemia called megaloblastic anemia. However, it is quite easy to combat as the sources of this vitamins are easily obtainable such as from eggs, cheese, and milk. If there's a relationship between those two, it could be the fact that B12 increases blood volume and contributes to hypertension but based on what I have learnt before, I've never come across of the correlation between these two entities.
Good job!
I have a friend who studied pharmacy.. And she was always telling me about pharmacology. I couldn't find it easy to understand. But from what I see here it is quite complex like she said.
Well done
My friends told me that Pharmacology is boring but I beg to differ. hahaha. Pharmacology is the main core of Pharmacy. It's quite complicated to understand but after knowing about how it happens and etc, the info will retain much longer in your brain. Thank you for the comment :)
Hmm that is true. Knowledge stays with the person.
You are very much welcome.
I've studied biomedical science and environmental toxicology. I considered being a medicinal chemist or pharmacist, so I still read pharmacological literature out of interest. Probably because as my wife & I get older, we need to be better informed about meds!
Congratulations @soulesque! You have completed some achievement on Steemit and have been rewarded with new badge(s) :
Click on any badge to view your own Board of Honor on SteemitBoard.
To support your work, I also upvoted your post!
For more information about SteemitBoard, click here
If you no longer want to receive notifications, reply to this comment with the word
STOPDo not miss the last announcement from @steemitboard!
many thanks for your information is great to know the big problems that hipertensión could give you if you do not take action when you are young or not take a good diet solutions or make some physical activities.
No problem @galberto . Despite of all the long winded post and discussions regarding anti-hypertensive medications, the very first basic step that everyone is afford to take is by adjusting their lifestyles to be healthier. Avoid excessive salt consumption, and exercise regularly !
Hi, soulesque! I just resteemed your post!
I can also re-steem and upvote some of your other posts for just 0.02 SBD/Steem if you are following me for 10 minutes
Check out @resteemyou's' introduction post
that's great, than you for the informations :)
Your welcome @benainouna :)
Stunning explanation about hypertension and pharmatical therapy.
Thank you @alzamna :)