Calibrating the PCR Tests
In the early stages of the covid pandemic novel PCR tests were rolled out and quickly became important diagnostic tools in the fight against this supposedly novel disease. Three years on and the PCR test is now considered the gold standard for COVID-19:
The gold-standard method for establishing a microbiological diagnosis of COVID-19 is reverse-transcriptase polymerase chain reaction (RT-PCR). ―Oliveira et al 1
But this was not always the case:
This study aimed to determine the sensitivity and specificity of reverse transcription PCR (RT-PCR) testing of upper respiratory tract samples from hospitalised patients with coronavirus disease 2019 (COVID-19), compared to the gold standard of a clinical diagnosis. ―Williams et al 1
The question is: How were these PCR tests calibrated in the first place?
Background Science
To properly understand this subject, it is first necessary to study some of the fundamental principles underpinning the science of diagnostic testing.
Condition Positive (P) The number of positive cases in the population being tested. A positive case means an individual who actually has the disease being tested for, irrespective of the result of their test.
Condition Negative (N) The number of negative cases in the population being tested. A negative case means an individual who does not have the disease being tested for, irrespective of the result of their test.
Prevalence The proportion of the population being tested that has the disease. If P individuals have the disease and N individuals do not have the disease, then by definition the Prevalence = P/(P+N).
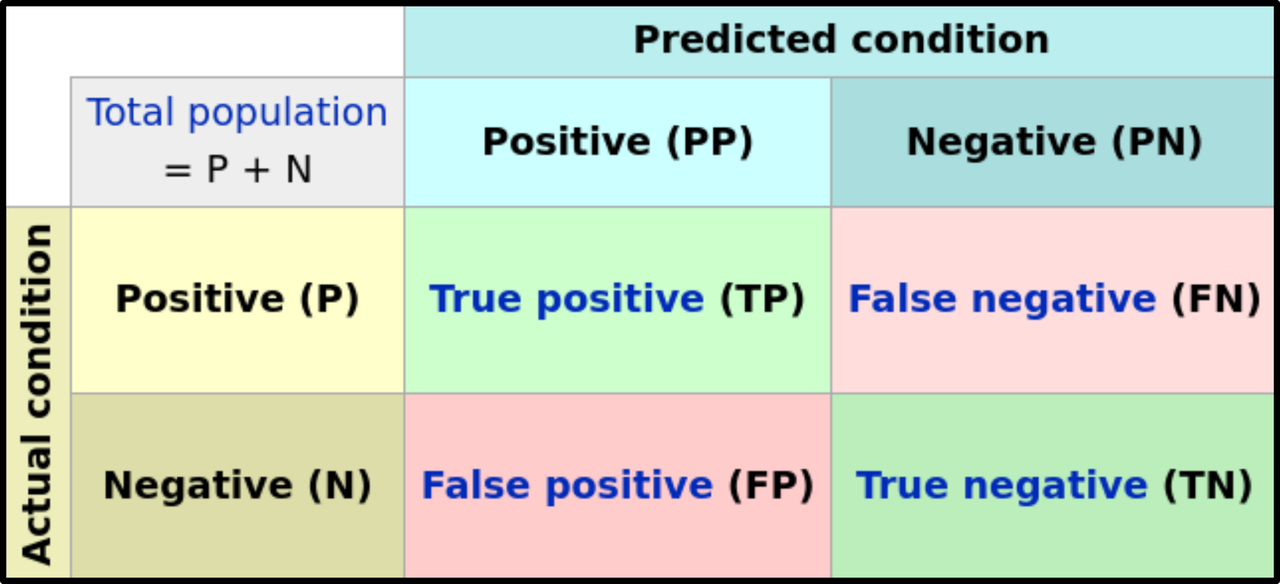
Four Cases
For every diagnostic test there are four possible outcomes, two of which involves errors:
True Positives (TP) Positive cases of the disease that are correctly diagnosed by the test as positive.
True Negatives (TN) Negative cases of the disease that are correctly diagnosed by the test as negative.
False Positives (FP) Negative cases of the disease that are incorrectly diagnosed by the test as positive. These are also known as Type I Errors.
False Negatives (FN) Positive cases of the disease that are incorrectly diagnosed by the test as negative. These are also known as Type II Errors.
These four cases are represented diagrammatically by a confusion matrix (see image above).
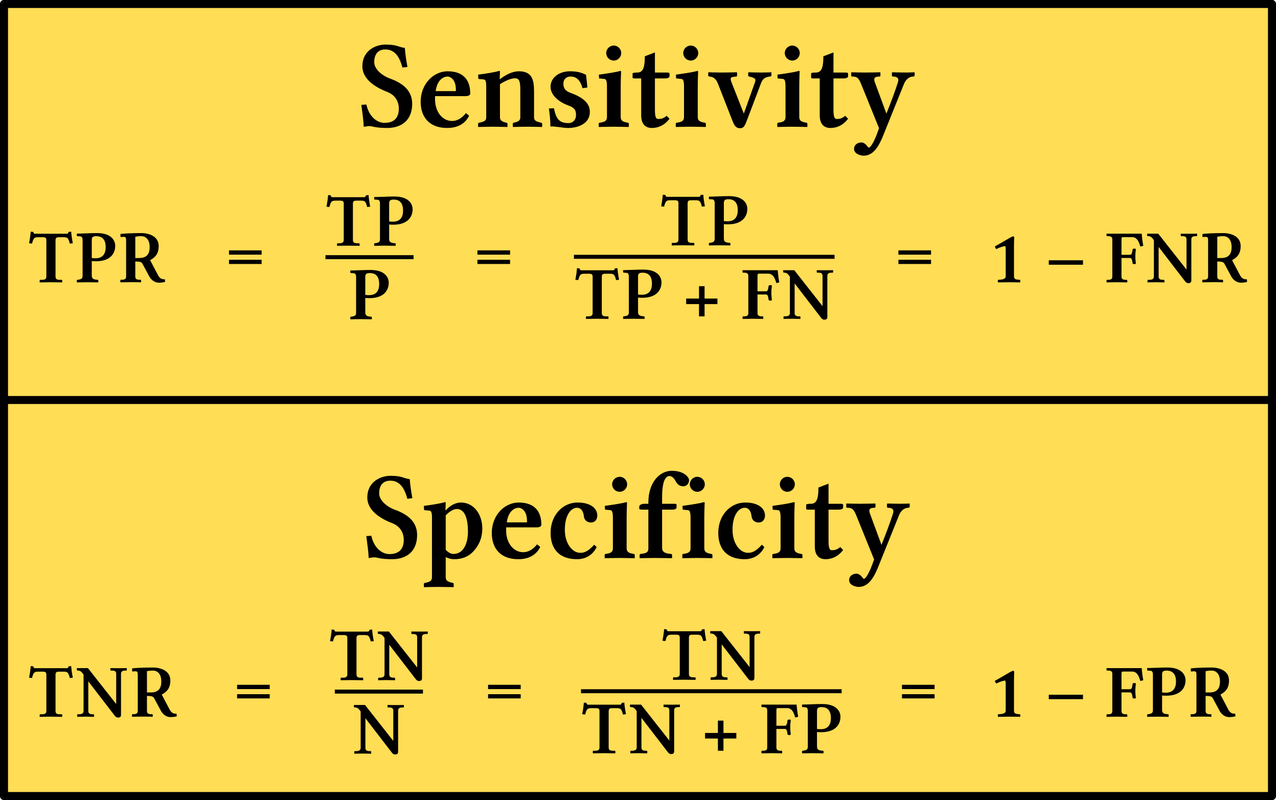
Sensitivity and Specificity
Two other important concepts to consider are those of sensitivity and specificity.
Sensitivity (TPR) The sensitivity of a diagnostic test measures the probability that it will correctly detect true positives. This is the true-positive rate. A highly sensitive test is one that is highly likely to correctly diagnose positive cases as positive. The downside to this is that it is also likely to be triggered by false cases, leading to several false positives. The term sensitivity refers to the fact that a highly sensitive test is easily triggered, even by negative cases. TPR = TP/P.
Specificity (TNR) The specificity of a diagnostic test measures the probability that it will correctly detect true negatives. This is the true-negative rate. A highly specific test is one that is highly likely to correctly diagnose negative cases as negative. Or, to put it another way, it is highly unlikely to diagnose a negative case as positive. The downside to this is that a highly specific test is not very sensitive. It is also likely to return a negative result in some positive cases, leading to false negatives. The term specificity refers to the fact that a highly specific test tends to be triggered only by the specific disease for which it is testing. TNR = TN/N.
In general, as the sensitivity of a test increases, its specificity decreases―and vice versa. The following hypothetical example illustrates this relationship. Imagine that a new medical disease has emerged. Two doctors, Peter & Paul, develop diagnostic tests to test for this disease.
Peter’s test is simply to return a positive result in all cases. Everyone who takes his test automatically test positive irrespective of their actual condition. This means that everyone who has the disease will be correctly diagnosed as positive. Therefore the true-positive rate is 100%. This is the sensitivity of Peter’s test. On the other hand, no one who does not have the disease will be correctly diagnosed as negative. Therefore the true-negative rate is 0%. This is the specificity of Peter’s test.
Paul’s test is simply to return a negative result in all cases. Everyone who takes his test automatically tests negative irrespective of their actual condition. This means that everyone who has the disease will be incorrectly diagnosed as negative. Therefore the true-positive rate is 0%. This is the sensitivity of Peter’s test. On the other hand, everyone who does not have the disease will be correctly diagnosed as negative. Therefore the true-negative rate is 100%. This is the specificity of Peter’s test.
Of course, this is a wholly unrealistic example. In reality, there will be a sort of trade-off between sensitivity and specificity, but both will tend to be quite high. For example, most rapid strep tests are alleged to have sensitivities of 90–95% and specificities of 98–99%.
Calibrating a Medical Test
In order to calibrate a new medical test for a particular disease it is first imperative that we have some independent way of testing for the disease―a gold standard (also known as a criterion standard) that can be trusted. Typically, the gold standard is the most reliable diagnostic test available, irrespective of cost or time.
Ideally, a gold standard test should have a sensitivity of 100% and a specificity of 100%. In other words, it ought to be infallible when diagnosing the disease in question. All positives detected by the gold standard are true positives, and all negatives are true negatives. In practice, gold standard tests usually fall short of this ideal.
How, then, does one calibrate a diagnostic test in the ideal case of a disease for which there exists a perfect gold standard? This is the procedure to be followed:
A large population of subjects is tested using the gold standard―the larger the better. The subjects are divided into two subpopulations based on the test results: P subjects who definitely have the disease : N subjects who definitely do not have the disease.
The P population is tested using the new diagnostic test that is being calibrated. The number of positives returned is TP, as these are true positives. Therefore the sensitivity of the test, the true-positive rate, is: TPR = TP/P.
The N population is tested using the new diagnostic test. The number of positives returned is FP, as these are false positive. The number of true negatives, then, is N–FP. Therefore the specificity of the test, the true-negative rate, is: TNR = (N–FP)/N.
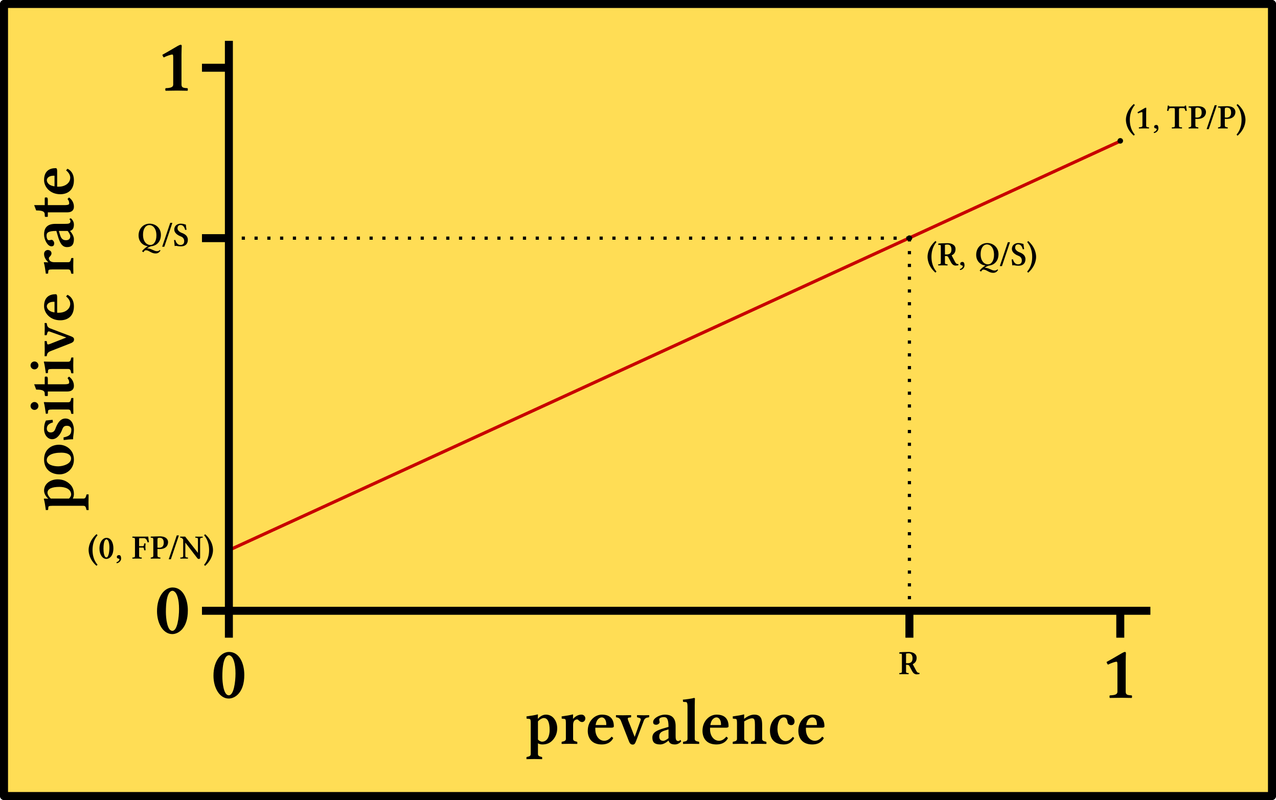
These two results are now plotted on a graph:
The x-axis measures the prevalence of the disease in the population being tested. The scale on this axis runs from 0 (no one has the disease) to 1 (everyone has the disease).
The y-axis measures the proportion of the population that tests positive. The scale on the y-axis also runs from 0 (no one tests positive) to 1 (everyone tests positive).
On this graph we plot the two points:
(1, TP/P)
(0 FP/N)
These two points are joined by a straight line. This line represents all possible outcomes when any given population is tested for the disease. This is because the relationship between the prevalence of the disease in a population and the proportion of positive tests returned (both true positives and false positives) when the whole of this population is tested is a linear one. This can be proved with some elementary linear algebra.
This graph can now be used to estimate the prevalence of the disease among a given population. A random and representative sample of S subjects is selected from the population. These are tested for the disease. Let’s say that Q positives are returned. These include both true positives and false positives. The proportion of positive tests is therefore Q/S. The point on the line with this as its y-coordinate is located. The x-coordinate of this point, R, is the prevalence of the disease:
Gold Standard for COVID-19
In order to properly calibrate a PCR test for covid-19 it is first necessary to develop a gold standard for covid-19. This is where the science of the PCR tests comes up against an inconvenient fact: there is no gold standard for covid-19.
Mike Stone, the independent researcher behind the online site known as ViroLIEgy, has recently examined this problem in some detail. He begins his study by asking a simple question: What is COVID-19?
... a disease is said to be defined by specific signs and symptoms ... In order to answer the question as to whether there are any new and/or specific signs or symptoms related to “Covid” that allow the disease to be easily defined as something new, we must start at the beginning. The world was first alerted to the presence of a pneumonia of unknown cause coming from China by the WHO on January 5th, 2020. In the statement, the WHO admitted that no causative agent had been identified and that the symptoms experienced in these cases were common, especially during the winter months. In other words, the only reason for the alert was that no cause through testing could be associated with these cases of typical pneumonia ...
Turning to the initial studies from China, we can glean some more information as to what these common symptoms were that necessitated an alert by the WHO. According to the Fan Wu et al. paper that provided the genome of the computer-generated “virus” that was eventually blamed as the cause, the 41-year-old patient the genome was obtained from suffered the non-specific symptoms of fever, dizziness, and a cough ... A companion study by Zhou et al. stated that the main symptoms experienced by the initial patients were fever, headache, dry cough, difficulty breathing, and pneumonia ... A related study by Zhu et al. examined three early patients presenting with pneumonia of an unknown cause. Symptoms were only available for two of the patients, and these included fever, cough, and chest discomfort ...
Thus, we can clearly see that there was nothing unusual about the symptoms experienced at the time “Covid” began to make the headlines. The disease that all of the patients were said to be suffering from was a pneumonia of an “unknown cause” presenting with common symptoms such as fever, cough, headache, dizziness, and difficulty breathing. There were absolutely no distinguishing signs or symptoms differentiating a “Covid” case from anyone suffering these same symptoms of disease other than the presumed “novel” cause ...
Thus, we can clearly see that there was nothing unusual about the symptoms experienced at the time “Covid” began to make the headlines. The disease that all of the patients were said to be suffering from was a pneumonia of an “unknown cause” presenting with common symptoms such as fever, cough, headache, dizziness, and difficulty breathing. There were absolutely no distinguishing signs or symptoms differentiating a “Covid” case from anyone suffering these same symptoms of disease other than the presumed “novel” cause. ―Mike Stone
As time passed and more cases of respiratory illness were diagnosed as covid, the list of symptoms grew. In short, any symptom displayed by anyone diagnosed with covid was assumed to be a symptom of this new disease known as COVID-19 and was accordingly added to the list. One of these symptoms was the loss of one’s sense of smell or taste, even though none of the Chinese paper that introduced covid to the world ever mentioned any such symptom:
... many believe that an acute loss of smell and taste is a new feature that is specific to “Covid.” A media frenzy promoting this as a new sign of the disease became ingrained in the collective consciousness when reports of positive patients experiencing these symptoms began circulating in March 2020. Originally, common indicators such as a fever, cough, and shortness of breath were the main warning signs that we were supposed to look out for if anyone feared that they had “Covid.” However, in late April 2020, the CDC added six more symptoms under the “Covid” umbrella as mass testing began to roll out. These included chills, repeated shaking with chills, muscle pain, headache, sore throat and new loss of taste or smell. In a clever case of subliminal messaging, the word new was often put in front of “loss of taste and smell” as a way to implant the idea that this occurrence was previously unheard of ... ―Mike Stone
But this is simply not true:
However, for anyone doing a cursory bit of research outside of the mainstream propaganda, it was abundantly clear that the loss of smell and taste were not new symptoms of disease nor were they specific to “Covid-19.” These symptoms are often associated with allergies, the common cold, influenza, drug reactions, head injuries, old age, etc. In an April 2020 interview with experts in anosmia, VCU School of Medicine faculty Richard Costanzo, Ph.D. and Evan Reiter, M.D., it is said that many people experience these symptoms without ever noticing that they are present until someone alerts them to it. Both men stated that it is a common occurrence and that there are many potential causes ...
While still highlighting loss of smell and taste as a potential sign of a “Covid infection,” an article from PositiveMed.com also pointed out that this is not a specific, nor a uniquely distinctive feature of “Covid,” and that it is actually quite common in respiratory disease ―Mike Stone
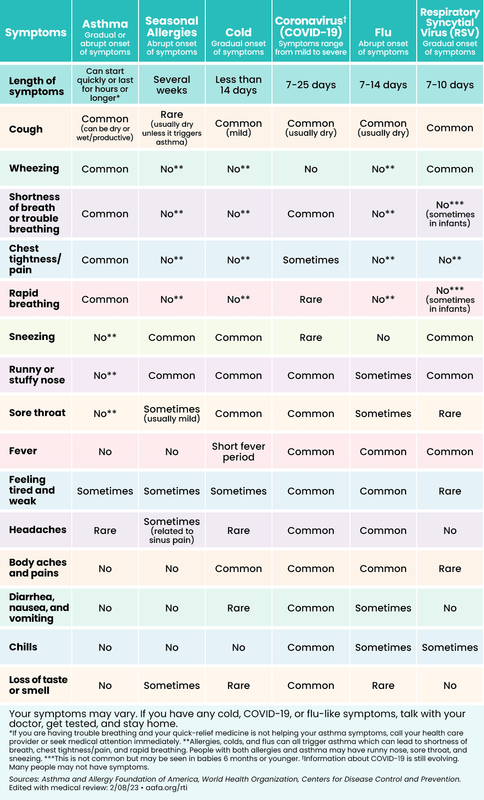
How, then, can a true case of this novel respiratory disease be distinguished from well-established respiratory diseases, such as influenza, the common cold, and pneumonia? The short answer is that covid cannot be distinguished from other common respiratory illnesses:
Even though COVID-19 manifests with different symptoms, none of these symptoms are present in every patient and there are no specific signs or symptoms that could suggest COVID-19 compared to symptoms and signs of respiratory illnesses caused by other viruses,such as influenza and common cold. ―Abebe et al, The newly emerged COVID-19 disease: a systemic review (2020)
The symptoms expressed by COVID-19 patients are nonspecific and cannot be used for an accurate diagnosis. Guan et al. reported that 44% of 1099 COVID-19 patients from China had a fever when they entered the hospital and that 89% developed a fever while in hospital. They further found that patients had a cough (68%), fatigue (38%), sputum production (34%), and shortness of breath (19%). Many of these symptoms could be associated with other respiratory infections. ―Udugama et al, Diagnosing COVID-19: The Disease and Tools for Detection (2020)
This inability to distinguish between covid and other respiratory illnesses on the basis of symptoms extends to other methods of clinical diagnosis:
The lack of specificity and an inability to diagnose a “Covid” case clinically is supported by a September 2021 [Fistera et al] study that attempted to create a differential diagnosis between “Covid” and other diseases. The authors concluded that “Covid” can not be differentiated from other respiratory infections via clinical signs, symptoms, or laboratory results. The symptoms defining “Covid” are non-specific and overlapped with many other conditions. The researchers admitted that establishing differential diagnosis criteria remained very challenging and that clinical discrimination was unreliable as there were no clinical or laboratory parameters that could be relied upon. ―Mike Stone
Without a gold standard to diagnose covid, how can any test for this “novel” disease be calibrated?
Mike Stone’s conclusion at the end of his lengthy and meticulously researched article is devastating:
When we break down what “Covid-19” truly is, it is no wonder why so many people have trouble defining and explaining how “Covid” is a new disease. There is absolutely no evidence that a new disease exists. What we have is a new label for the same symptoms seen every single year that are regularly presented under various other labels. “Covid-19” is simply the latest name to enter the ring. As there are no defining signs and symptoms and there is no way to identify “Covid” based upon clinical, laboratory, or histopathological methods, it falls upon the fraudulent PCR tests to diagnose a “Covid” case. This was admitted by the CDC when they stated that illnesses such as the flu and “Covid” can not be differentiated via symptoms alone, thus requiring PCR tests for diagnosis ...
“Covid-19” truly is nothing but a positive PCR result. That’s it. This is why a “new disease” called “Covid-19” can be found mostly in the asymptomatic, i.e. healthy people who are not suffering from any disease whatsoever. This is why the symptoms belonging to “Covid” can range from none to the common cold, to Kawasaki disease, to frost bite, and all the way to death. This is why the CDC was able to add six “new” symptoms to “Covid” in April 2020, over four months after the common symptoms of pneumonia were first identified in patients in China, upon the introduction of mass testing. When one is labelled as a “Covid” case based upon a fraudulent test, any symptoms that they may or may not experience as well as any underlying health conditions that they may have had, become absorbed into the “Covid” umbrella ...
As “Covid” cannot be diagnosed clinically based upon specific signs and symptoms, there is no way to get an accurate disease prevalence rate in order to determine the accuracy of the PCR result. Thus, PCR is used to generate cases in order to calculate disease prevalence so that its results can be claimed as accurate. However, PCR cannot be used to create cases in order to determine its own accuracy. This is outright fraud, and it is the very reason why there was never any “viral pandemic.” It has always been, and will continue to be, a testing pandemic until enough people become aware of the truth and stop testing for a “new disease” that never existed in the first place. ―Mike Stone
The extent of this fraud cannot be overemphasized. Without a gold standard for COVID-19, it is simply not possible to calibrate a PCR test in the first place. And yet we have somehow reached the position where PCR is now considered the gold standard for COVID-19, with an assumed sensitivity of 100%:
A positive COVID-19 PCR test means that SARS-CoV-2 is present. A negative result could either mean that the sample did not contain any virus or that there is too little viral genetic material in the sample to be detected. ―NIH: National Human Genome Research Institute
And that’s a good place to stop.
References
- Endeshaw Chekol Abebe et al, The Newly Emerged COVID-19 Disease: A Systemic Review, Virology Journal, Volume 17, Article 96, BioMed Central, Springer Nature, London (2020)
- Mirella Cristine Oliveira et al, Diagnostic Accuracy of a Set of Clinical and Radiological Criteria for Screening of COVID-19 Using RT-PCR as the Reference Standard, BMC Pulmonary Medicine, Volume 23, Article 81, BioMed Central, Springer Nature, London (2023)
- Buddhisha Udugama et al, Diagnosing COVID-19: The Disease and Tools for Detection, ACS Nano, Volume 14, Issue 4, Pages 3822–3855, American Chemical Society, Washington, DC (2020)
- Thomas C Williams et al, Sensitivity of RT-PCR Testing of Upper Respiratory Tract Samples for SARS-CoV-2 in Hospitalised Patients: A Retrospective Cohort Study, Wellcome Open Research, Wellcome Trust, London (2022)
Image Credits
- COVID-19 Poster: © 2021 Dublin Region Homeless Executive, Fair Use
- Gold Standard: © The Atlantic Monthly Group, Creative Commons License
- Mike Stone: © Tom Cowan, Fair Use
- Richard Costanzo & Evan Reiter: © VCU Health, Fair Use
- Kary Mullis: Jim Wilson (photographer), © The New York Times, Redux Pictures, Fair Use
- Symptoms of Common Respiratory Illnesses: © Asthma and Allergy Foundation of America, Fair Use
Online Resources
