Pathogenesis of Drepanocytosis (Sickle Cell Anemia) / Patogenesi della Drepanocitosi (Anemia Falciforme)
Hello to all dear friends, in the last column we have reviewed the mutations, studied the molecular bases of B-thalassemia and studied its pathogenetic path, if you missed it you will find all this at the following link
Genetic mutations as a cause of disease (B-thalassaemias)
Today we will explore the pathogenetic pathway of another genetic-based pathology that affects hemogobline, drepanocytosis, or better known as sickle-cell anemia, good reading.
Pathogenesis of Drepanocytosis (Sickle Cell Anemia)
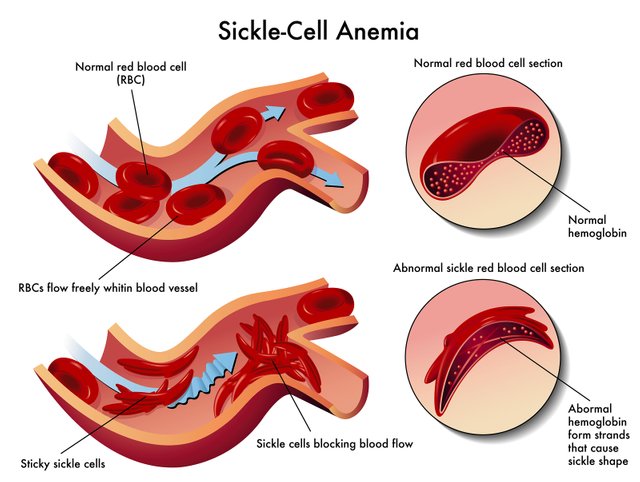
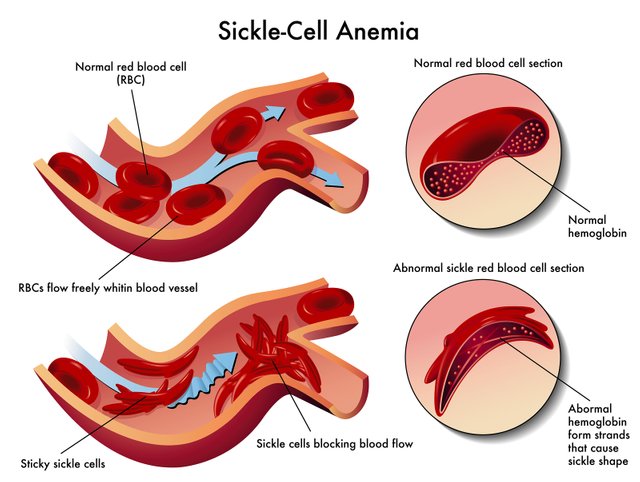
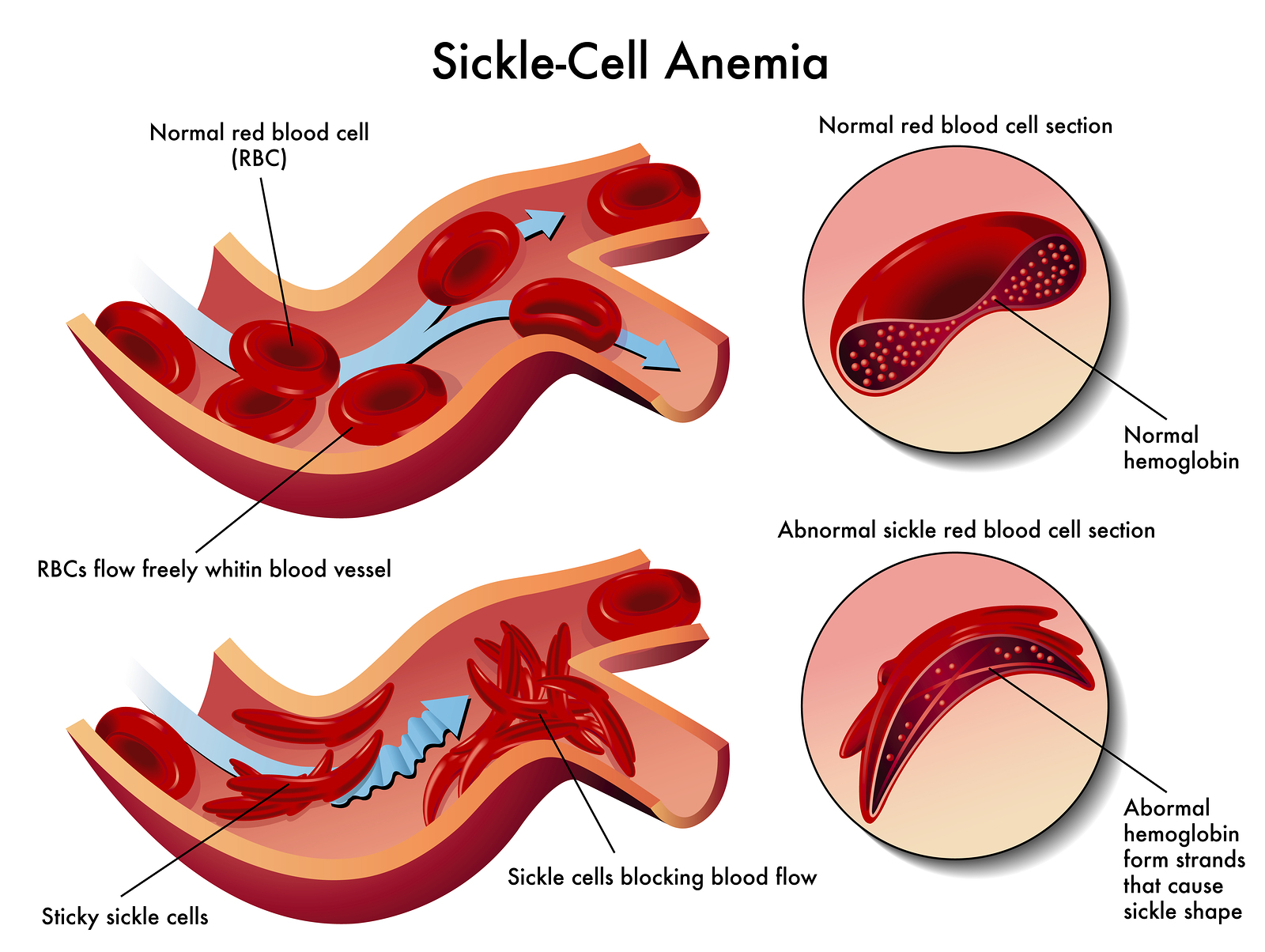
Drepanocytosis or sickle-cell anemia is a type of anemia characterized by the presence of red blood cells in the shape of a sickle.
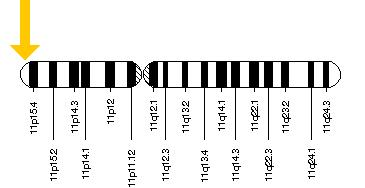
It is determined by a point mutation to codon number 6 of the β globins gene, which is placed on an exon.
The mutation results in a non-preservative substitution of the amino acid glutamate by a valine on the chain
nascent peptide.
The hemoglobin with the β-chain so altered is called HbS. When it is bound to oxygen, it is totally
identical to HbA; when HbS releases oxygen at the peripheral level it becomes insoluble and then falls into the red blood cell.
Aggregating in paracrystalline structures called tactoids. Tactoids stress and lengthen the form of the
red blood cell making it into a scythe shape. The mutation therefore determines a quantitative alteration
of circulating hemoglobin, which, however, turns the disease into a quantitative alteration, since the red blood cells
scythemyces are apoptosis or are destroyed by hemocateretic organs (liver and spleen)
Drepanocytosis differs from β-thalassemia for the initial stages of the pathogenesis, in fact sickle-cell anemia expresses its
effects already at secondary level only in venous environment, at tissue level, where low pO2 is present.
To analyze the
pathogenesis of this pathology it is useful to follow the path that the erythrocytes of a drepanocytotic make in a circle.
In the bone marrow the erythroblasts carry bound haemoglobin S (HbS). Since the marrow is an extremely
oxygenated, erythroblasts form and mature normally because an HbS is assembled within them.
oxygenated, so perfectly soluble.The erythroblasts at this point enter the bloodstream and reach the lung,
where oxygen is present in large quantities, so the erythrocyte maintains its normal lenticular form.At the level
cardiac, despite being subjected to great elastic and mechanical stress, the erythrocytes continue their course to
get to the suburbs.Once they reach the peripheral organs, the erythrocytes give up the O2, the tactoids are formed, and they assume the
scythe shape. These scythe-shaped erythrocytes lose their elasticity and can no longer pass the blood microcirculation: a
capillary level, they rupture, causing peripheral hyperhemolysis (leading to anaemia) and hypoxia, since they cause a blockage of the blood circulation.
circulation causing metabolic shift, i.e. abnormal production of lactic acid.The accumulation of lactic acid,
associated with hypoxia, determines tissue necrosis that stimulates the nociceptive transmissions of the CNS, causing pain (vasocclusive crises).
Necrosis and hypoxia are closely related and the basis of organ microinfarcts, initially confined to an area
small. A micro infarction, is completely subclinical, as it does not give any obvious effect; however, the
organs of a patient suffering from drepanocytosis suffer a large number of microinfarctions, which damage the organ
considered and aggravate the necrosis.
In addition, the phenomenon of necrosis also implies the presence of inflammation, with
formation of oedema (which further compresses the tissue capillaries) and conglutination of blood (detectable parameter
with ESR): these events amplify the heart attack zone.
In this picture of strong anemia, a reduced part of red blood cells can come back into circulation from the periphery and reach
the hemocateretic organs such as the spleen and liver.
In the early stages of sickle-cell anemia there is an increased function of
hematosplenomegaly cause hematosplenomegaly. However, subsequently, the microinfarcts given by hemolysis increase and
conglutination: these are the cause of necrosis, inflammation and subsequent connectification of the tissue, which leads to
to atrophy. At macroscopic level, in fact, the spleen becomes atrophic and manifests the appearance of black spots, an index of necrosis.
If finally the erythroblasts manage to return to the pulmonary level, they are reoxygenated, and in this way the
phenomenon of structural and functional recovery of the red blood cell, resuming the circle.
Introduzione
Ciao a tutti cari Amici, nell'ultima rubrica abbiamo ripassato le mutazioni, studiato le basi molecolari della B-Talassemia e studiato il suo percorso patogenetico, se ve la siete persa troverete tutto questo al seguente link
Genetic mutations as a cause of disease (B-thalassaemias)
Oggi esploreremo il percorso patogenetico di un altra patologia a base genetica che colpisce l'emogoblina, la drepanocitosi, o più conosciuta come anemia falciforme, buona lettura.
Patogenesi della Drepanocitosi (Anemia Falciforme)
La drepanocitosi o anemia falciforme è un tipo di anemia caratterizzato dalla presenza di globuli rossi con la forma a falce.
E’ determinata da una mutazione puntiforme al codone numero 6 del gene per le β globine, che è posizionato su un esone.
La mutazione determina una sostituzione non conservativa dell’aminoacido glutammato con una valina sulla catena
peptidica nascente.
L’emoglobina con le catene β così alterate prende il nome di HbS. Quando questa è legata all’ossigeno risulta totalmente
identica all’HbA; quando l’HbS cede l’ossigeno a livello periferico diventa insolubile e quindi precipita all’interno del globulo rosso.
Aggregandosi in strutture paracristalline che prendono il nome di tactoidi. I tactoidi stressano e allungano la forma del
globulo rosso facendogli così assumere una forma a falce. La mutazione determina quindi un’alterazione quantitativa
dell’emoglobina circolante la quale tuttavia trasforma la patologia in alterazione quantitativa, in quanto i globuli rossi
falcemici vanno incontro ad apoptosi o vengono distrutti dagli organi emocateretici (fegato e milza)
La drepanocitosi differisce dalla β-talassemia per le fasi iniziali della patogenesi, infatti l’anemia falciforme esplica i suoi
effetti già a livello secondario solo in ambiente venoso, a livello tessutale, dove è presente una bassa pO2.
Per analizzare la
patogenesi di questa patologia è utile seguire il percorso che compiono in circolo gli eritrociti di un drepanocitotico.
Nel midollo osseo gli eritroblasti portano legata l’emoglobina S (HbS). Essendo il midollo un organo estremamente
ossigenato, gli eritroblasti si formano e maturano normalmente poiché all’interno di questi viene assemblata un’HbS
ossigenata, quindi perfettamente solubile.Gli eritroblasti a questo punto entrano in circolo e arrivano a livello polmonare,
dove l’ossigeno è presente in grandi quantità, quindi l’eritrocita mantiene la sua forma lenticolare normale.A livello
cardiaco, nonostante siano sottoposti a grandi stress elastici e meccanici, gli eritrociti proseguono il loro percorso fino ad
arrivare in periferia.Arrivati agli organi periferici, gli eritrociti cedono l’O2, si vengono a formare i tactoidi, e assumono la
forma a falce. Questi eritrociti falcemizzati perdono la loro elasticità e non riescono più a passare il microcircolo ematico: a
livello capillare, si rompono, causando iperemolisi periferica (che porta ad anemia) e ipossia, poiché determinano un blocco
della circolazione causa di shift metabolico, ovvero produzione abnorme di acido lattico.L’accumulo di acido lattico,
associato all’ipossia, determina necrosi tissutale che stimola le trasmissioni nocicettive del SNC, causando dolore (crisi vasocclusive).
La necrosi e l’ipossia sono strettamente correlate e alla base di microinfarti dell’organo, inizialmente circoscritti a un’area
di piccole dimensioni. Un microinfarto, è completamente subclinico, in quanto non dà nessun effetto evidente; tuttavia, gli
organi di un paziente affetto da drepanocitosi subiscono un grande numero di microinfarti, i quali danneggiano l’organo
considerato ed aggravano la necrosi.
Inoltre, il fenomeno di necrosi implica anche la presenza di infiammazione, con
formazione di edema (che comprime ulteriormente i capillari dei tessuti) e conglutinazione di emazie (parametro rilevabile
con VES): tali eventi amplificano la zona infartuata.
In questo quadro di forte anemia, una ridotta parte di globuli rossi riesce a tornare in circolo dalla periferia e raggiungono
gli organi emocateretici quali milza e fegato.
Nelle prime fasi di anemia falciforme si assiste ad aumentata funzione di
emocateresi causa di epatosplenomegalia. Tuttavia, successivamente, aumentano i microinfarti dati da emolisi e
conglutinamento: questi sono causa di necrosi, infiammazione e successiva connettivazione del tessuto, la quale conduce
ad atrofia. A livello macroscopico infatti, la milza diventa atrofica e manifesta la comparsa di macchie nere, indice di necrosi.
Se in ultimo gli eritroblasti riescono a tornare a livello polmonare vengono riossigenati, e in questo modo si determina il
fenomeno di recovery strutturale e funzionale del globulo rosso, riprendendo il circolo.
Fonti/Sources
Immagini/Pictures
{kind=link}
{kind=link}
Questo post è stato condiviso e votato all'interno del discord del team curatori di discovery-it.
This post was shared and voted inside the discord by the curators team of discovery-it
si tratta di quel tipo di anemia che non fa avere figli?...o che in passatonnon faceva avere figli??
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @minnowbooster.
If you appreciate the work we are doing, then consider supporting our witness @stem.witness. Additional witness support to the curie witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Please consider using the steemstem.io app and/or including @steemstem in the list of beneficiaries of this post. This could yield a stronger support from SteemSTEM.
Congratulations @riccc96! You have completed the following achievement on the Steem blockchain and have been rewarded with new badge(s) :
You can view your badges on your Steem Board and compare to others on the Steem Ranking
If you no longer want to receive notifications, reply to this comment with the word
STOP