An Original Research of Mine: Asymmetric Dimethylarginine Level May Predict the Severity of Coronary Heart Disease
Hello everyone,
I am very glad to have been writing in Steemit for more than five months. So far, I have written a lot about travel and culinary. From today on, I will write more about health and medicine since they are my area of expertise. Until now I am working as internist at Munyang Kute Redelong Hospital of Bener Meriah Dictrict in Aceh Province, Indonesia. By the way, let me introduce myself once more, my name is dr. Abdul Razak, SpPD, and my steemit account is @razack-pulo. I graduated from Sriwijaya University of Palembang, Indonesia. My registration number as an internist is 1611401316091980, and may be assesed here.

Well, today I am going to share my original research with the steemian around the world. I was conducting a study on 43 patients with coronary heart disease who underwent corangiography at Mohammad Hoesin Hospital, Palembang, Indonesia from November 2015 until January 2016. I was searching for correlations between serum ADMA levels and the serverity of Coronary Heard Disease (CHD) measured by Gensini Score.
As we know that coronary heart disease (CHD) remains a major health problem in the world because of its morbidity and mortality. One of the methods for establishing a diagnosis of CHD is by coronary angiography, it is to find the presence of coronary arterial stenosis.
Gensini score is one of the most widely used scoring systems to determine the severity of CHD stenosis. In addition to Gensini score, it can be also measured by the SYNTAX score, or the CASS-50 score. While Asymmetric dimethylarginine (ADMA) is a structural analog of L-arginine, competitively inhibits the enzyme NO synthase and thus it has role in endothelial disfunction. Studies show that serum ADMA has independent association with the presence and severity of CHD. I am interested in doing this research because there is no research in Indonesia, especially Palembang. There is still no publication of this study in Indonesia and especially in Palembang.
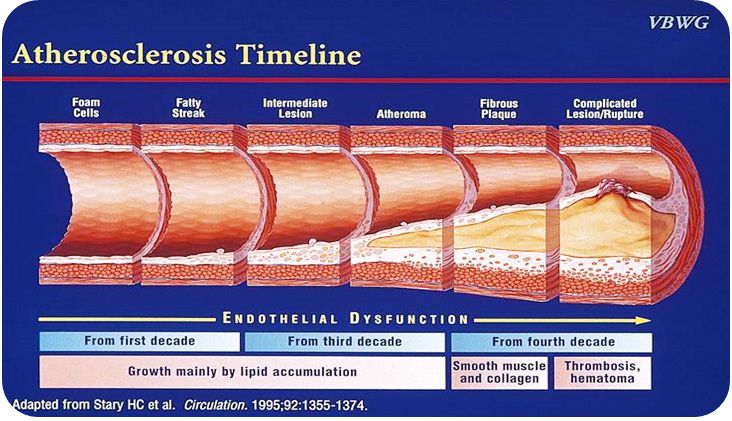
Atherosclerosis in the coronary arteries causes angina pectoris and myocardial infarction. Atherosclerotic plaque in CHD causes stenosis in coronary arteries to inhibit or reduce blood flow through the affected blood vessels. A reduced blood flow causes myocardial ischemia, angina pectoris or myocardial infarction.
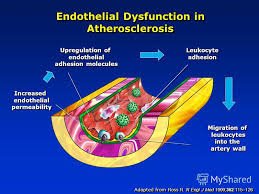
Endothelium plays an important role in vascular homeostasis that secretes a number of regulatory materials to maintain vascular tone. The damaged endothelium may not perform its function properly. This is a preliminary occurrence of atherosclerosis. Among these regulatory agents, Nitric Oxide (NO) is the most important vasodilator material released by endothelium. Additionally, NO also inhibits platelet adhesion and aggregation, adhesion of monocyte and leukocytes in the endothelium, vascular smooth muscle cell proliferation and low-density lipoprotein (LDL) oxidation. If there is a breakdown in NO bioavailability it will interfere with all these functions to trigger further atherosclerosis and progression. Nitric oxide, an anti-Endogenous atherogenic is produced from L-arginine by endothelial Nitric Oxide synthase (eNOS). eNOS requires molecular oxygen and various cofactors. Any condition that reduces endothelial NO production will cause atherosclerosis.
Asymmetric dimethylarginine (ADMA) is an L-arginine analog that acts as an endogenous competitive inhibitor of eNOS and contributes to endothelial dysfunction. Serum ADMA levels are elevated in patients with cardiovascular risk factors such as hypertension, diabetes mellitus, hypercholesterolemia, and hyperhomocysteinaemia. Many studies have shown that high baseline ADMA is a predictor of poor prognosis in patients with stable angina pectoris, unstable angina pectoris and CHD as demonstrated in Tse Min et al., Schnabel et al and Tanja K et al.
Previous studies have shown a strong association between serum and CHD levels, as in Schulze F et al., showed that serum ADMA levels were higher in patients with CHD than in healthy controls. In addition, Valkonen et al found a significant increase in risk CHD in middle-age men who do not smoke, where serum ADMA levels are high. In addition, a new study by Lu et al showed that patients with stable coronary heart disease, ADMA is also an independent risk factor for cardiovascular disease.
[Source: Taken fron ref No 10)
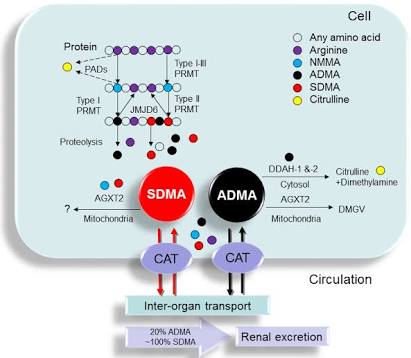
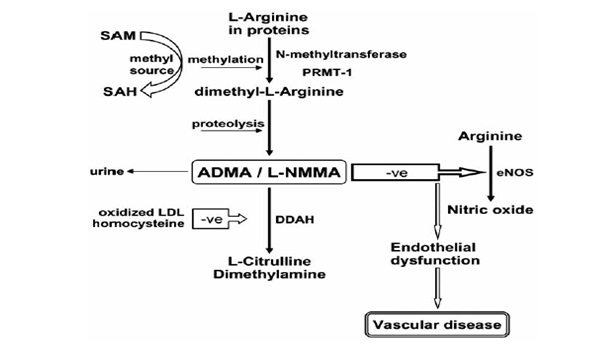
The figure above shows the synthesis pathway and metabolism of ADMA where methylation of arginine residues inside the peptide occurs via Nmethyltransferases, arginine N-methyltransferase-1 protein (PRMT-1). S-adenosylmethionine (SAM) is a methyl donor, which turns into S-adenosylhomocysteine (SAH). The breakdown of proteolytic proteins produces ADMA and N-monomethyl-L-arginine (LNMMA) in cells, and can be found in the circulation. ADMA is an inhibitor of endothelial nitric oxide synthase (eNOS) that competes with its L-arginine substrate, thus disrupting the production of nitric oxide (NO), resulting in endothelial dysfunction and ultimately leading to atherosclerosis. ADMA is partially eliminated through urine and mostly by metabolism by dimethylarginine dimethylaminohydrolase (DDAH) enzyme into citrulline and dimethylamine.
This research was conducted by using Correlative analytic design method with a prospective approach without control.
After doing the research, I finally got the following results:
There were 43 subjects with 25 male (79,1%). The mean level of serum ADMA was 0,50±0,10 µmol/L and its cut off point was 0,50 µmol/L. There was relationship among sex (p=0,019), smoking (p=0,005), serum ADMA (p=0,002) and the degree of coronary arterial stenosis. While other risk factors such as age, BMI, hypertension, diabetes, and dislipidemia had not found any relationship. Statistical analysis showed significantly moderate correlation between serum ADMA level and the degree of coronary arterial stenosis measured by Gensini score (r=0,414; p=0,006).
And the conclusion: there is significantly moderate correlation between serum ADMA level and the degree of coronary arterial stenosis measured by Gensini score in CHD patients at Mohammad Hoesin General Hospital Palembang, Indonesia.
Reference list;
- World Health Organization (WHO). Cardiovascular Diseases. Geneva, WHO Press:2015
- Boudi BF. Risk factors for coronary artery disease. Avaialabe at www.emedicine.medscape.com
- Sheridan PJ, Crossman DC. Critical review of unstable angina and non-ST elevation myocardial infarction. Postgraduate Med J. 2002; 78: 717–26
- Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005; 352:1685-95
- Neeland IJ, Patel RS, Eshtehardi P. Coronary angiographic scoring systems: an evaluation of their equivalene and validity. Am Heart J. 2012;164(4):547-52
- Chen Zw, Chen YH, Qian JY. Validation of a novel clinical prediction score for severe coronary artery diseases before elective coronary angiography. PloS ONE. 2014; 9(4):1-8
- Can F, Ziyrek M, Erdem S, Civan M, Gormus U, Sahin S, et al. The association between coronary atherosclerotic burden and asymmetric dimethylarginine, carotis intima media thickness and endothelial function. Türk Kardiyol Dern Arş - Arch Turk Soc Cardiol. 2014;42(8):701-09
- Antman EM, Selwyn AP, Braunwald E, Loscalzo J. Ischemic heart disease. Harrison’s Principles Of Internal Medicine. 17th Ed. Philadelphia: The McGraw-Hill Companies;2012.p.1514-27
- Stephen F, Gross GJ. Coronary blood flow and myocardial ischaemia. In Fuster V, Walsh RA, O'Rourke RA, Poole-Wilson P. Hurst’s The Heart. 12th Ed. Philadelphia: The McGraw-Hill Companies;2008:p.1259-76
- Badimon JJ. Coronary thrombosis: local & systemic factors. In: Fuster V, Walsh RA, O'Rourke RA, Poole-Wilson P, editors. Hurst’s The Heart. 12th Ed. Philadelphia: The McGraw-Hill Companies;2008:p.1245-58
- Kerkeni M, Addad F. Hyperhomocysteinemia, endothelial nitric oxide synthase polymorphism, and risk of coronary artery disease; Clinical Chemistry. 2006;52: 153-58
- Kuhlencordt PJ, Gyurko R, Han F, Crosbie MS. Accelerated atherosclerosis, aortic aneurysm formation, and ischemic heart disease in apolipoprotein endothelial nitric oxide Synthase double-knockout. Circulation. 2001; 104:448-54
- Boger RH. The emerging role of asymmetric dimethylarginine as a novel cardiovascular risk factor. Cardiovasc Res. 2003; 59(4):824-33
- Shivkar RR, Abhang SA. Ratio of serum asymmetric dimethyl arginine (ADMA)/ nitric oxide in coronary artery disease patients. Journal of Clinical and Diagnostic Research. 2014;8(8):4-6
- Vallance P, Leone A, Calver A, Collier J, Moncada S. Accumulation of an endogenous inhibitor of NO synthesis in chronic renal failure. Lancet. 1992;339:572-75
- Krempl TK, Maas R, Sydow K, Meinertz T. Elevation of asymmetric dimethylarginine in patients with unstable angina and recurrent cardiovascular events. Eur Heart J. 2005; 26(18):1846-51
- Schulze F, Lenzen H, Hanefeld C. Asymmetric dimethylarginine is an independent risk factor for coronary heart disease: results from the multicenter Coronary Artery Risk Determination investigating the Influence of ADMA Concentration (CARDIAC) study. Am Heart J. 2006; 152:491-8
- Valkonen VP, Paiva H, Salonen JT. Risk of acute coronary events and serum concentration of asymmetrical dimethylarginine. Lancet.2001;358:2127-8.
- Zoccali C, Bode-Boger S, Mallamaci F. Plasma concentration of asymmetrical dimethylarginine and mortality in patients with end-stage renal disease: a prospective study. Lancet. 2001; 358:2113-7
- Sibal L, Agarwal SC, Home PD, Boger RH. The role of asymmetric dimethylarginine (ADMA) in endothelial dysfunction and cardiovascular disease. Current Cardiology Reviews.2010;6:82-90
Thank you, and warm regard from Indonesia
ABDUL RAZAK, MD or @razack-pulo
Internal Medicine Specialist [Internist]
Munyang Kute Redelong Hospital
Bener Meriah District of Aceh Province, Indonesia
Nyan ka hie dokter,
ka lon patis bereh that,
hana ilme kamoe inan lom dok.
Hahaha.. lage tapeugah malam nyan.. trims beh
Keren! Adikku ini dokter yang pintar banget dan teruskan risetnya untuk membantu semua!
Trimakasih kakakku @mariska.lubis.. hehehe Miss you :)
Menarik baca hasil risetnya pak dokter @razack-pulo. Akan tetapi jauh lebih menarik lagi jika bisa sharing sambil ngopi bersama para steemian. Karena penyakit jantung koroner sangat rentan bagi steemian :)
Sirip bang. InsyaAllah kalo ada di bireuen nanti kita ngopi :)
Siap! bang @razack-pulo
Bereh laju penjelasan droneh pak, jelas ju pak , bahaya tat penyakit jantong nyan . Salam dan sukses sabe pak .
Beutoi bang... mudah2an bermanfaat.. :)
Mantap dokter,informasi yang luar biasa,buat kami yang awam ini sangat bermanfaat ,menambah wawasan buat saya priadi dan buat para stemia semua tentang penyakit jantung koroner...
Moga bermanfaat bagi semua. Mudah2an tulisan2n berikutnya lebih baik dan lebih bermanfaat..
Mantap pak dokter. Terima kasih pak untuk postingannya.
Sama2 @agusscout :)
Good researche for science....
Mantap bg. Semoga sukses selalu....
Thank you very much
klw sering baca biokimia, mungkin agak ngerti la yah bg :)
Heheh. Jelas an
Ilmu kesehatan yang sangat bermanfaat, ini baru postingan super keren karena sesuai dengan profesi.. hehe
Hehe.. makasih atas dukungannya bang @mushthafakamal :)
Saya akan coba juga masukkan hasil penelitan saya hehee... good job @razack-pulo
Mantaaap bg. Bisa ditulis bang. Pasti keren..