Pathological fractures as a paraneoplastic expression
Pathological fractures, all those bone lesions (loss of bone continuity) originated spontaneously, product of a simple movement, excluding any traumatic cause.
The causes can be diverse from congenital diseases (osteogenesis imperfecta), to primary neoplasms or metastases, acquired bone disease (such as osteoporosis) and infections (osteomyelitis). In adults, this pathological entity is associated in more than 90% of cases with neoplastic pathologies, such as bone tumor, and metastatic lesions.
The skeletal system is the third one in frequent to present metastasis by a primary lesion, having in first and second place the lung and the liver.
The most commonly affected structures are the pelvis, skull, costal arches, vertebral bodies, and the femur. Fractures can be presented as: Oblique, Comminuted, Spiral, Composite or open, closed, impaction and avulsion.
Human Skeleton. Public domain image source maxpixel

Bone Structure
Our body is composed in the adult by 206 bone pieces, joined by joint systems formed by ligaments, tendons, articular discs, and synovial fluid, which allow the human body to maintain its architecture, providing protective function, support and execute complex and simple movements as the march.
{kind=link}
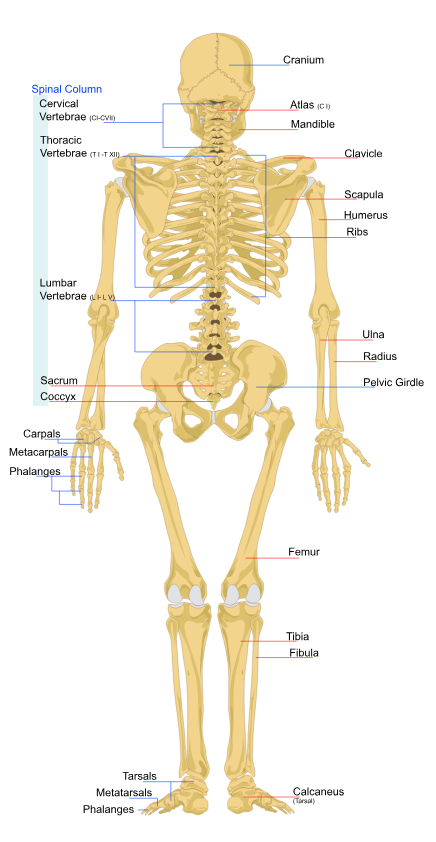
Diagram of a human female skeleton, back view. Public domain image source Wikipedia.
The present medical case is brought up for discussion, since in most of the cases, as in this case, the presence of pathological fractures is usually associated with paraneoplastic expressions, understood by this as the clinical manifestation resulting from a primary neoplastic lesion. not previously diagnosed.
Medic report
A 41-year-old male patient with no known medical history, who started the current disease about 2 years ago, characterized by muscular contracture and moderate to intense cervicalgia that calms with conventional NSAIDs and muscle relaxants. Clinical reappearance 2 months after lift large weight, paresthesia associated limbs, dysesthesia, decreased muscle strength to predominance of intermittent lower limbs, with movements not well coordinated, and volume increase in cervical region of about 5x5 cm painless, indurated without signs of phlogosis, plus of weight loss approximately 18 kg, two weeks ago dysphagia was associated with solids that progresses to liquids and dysphonia, reason for which it is valued and its admission is decided.
None of importance.
Positive for current illness: Alcohol, beer every weekend for 20 years, without drunkenness. Tobacco, cigarettes 1 daily box for 25 years IPA: 25.
Physical exam
Vital Signs:
Patient in stable general conditions, afebrile to the touch, hydrated, eupneic, tolerates ambient oxygen and orally only with liquids. Isochoric pupils normorreactives to light. ENT without alterations. At the level of the neck, there is a slight increase in volume in the occipital region of approximately 0.5 x 0.5mm soft, not painful without signs of phlogosis. No cervical adenopathy, neck stiffness and inability to lateralize (use of cervical immobilizer). Symmetric thorax, normoexpansible, apex in 5th intercostal space, mid clavicular line, RsCsRs without murmur, audible MVS without aggregates. Abdomen: flat, RsHsAs (+), soft, depressible, not painful to superficial or deep palpation, visceromegalies are not palpated. Male genitals, of normal appearance and configuration. Extremities: hypotrophic, without edema. Neurological: vigil, conscious, oriented in time, space and person, coherent and fluid language with mild dysphonia, without involvement of cranial nerves, muscle strength of upper and lower limbs IV / V, ROT in lower limbs, hyperreflexia and in upper normoreflex, sensitivity superficial and proprioceptive (+) and stereognotic (-), ataxic march, without signs of meningeal irritation.
Para-clinical
The positive is brought up for physical examination and current illness.
Complete hematology:
Blood chemistry:
Total and Free PSA: within normal parameters for age.
Peripheral blood smear:
Red Series: mild anisocytosis, with predominance of microcytosis, moderate hypochromia, mild poikilocytes.
White series: Neutrophilia, lymphopenia, presence of reactive lymphocytes, and hypo granulations in neutrophils.
Platelets: in normal quantity, presence of macroplates.
Sputum Bk
10/22/18 Not observed BAAR KOH: Positive for simple yeasts.
10/23/18 Not observed BAAR KOH: Negative.
Bk of urine
10/22/18: Not observed BAAR KOH: Negative.
Complementary studies
Thorax PA radiography:
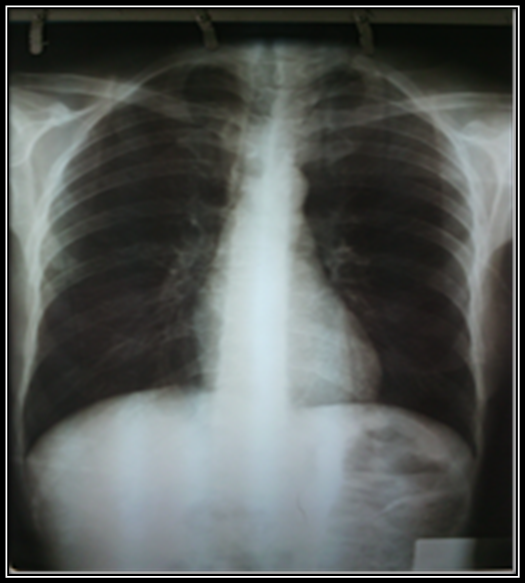
Conclusions: cardiac silhouette of normal size and shape, pulmonary fields without lesions. displacement of the first 3 vertebral bodies is observed.
Lateral X-ray of the cervical column:

Conclusions: it is evidenced at the level of the vertebral body C2 or Axis displacement towards the outside and crushing it with loss of the architecture of the rest of the cervical spine.
Ultrasound
Liver: normal size and shape. LHD: 15.3 cm.
Biliary tract: not dilated.
Gallbladder: little fulfilled due to lack of fasting.
Spleen: length 11cm.
Pancreas: without injuries.
Kidneys: symmetric, size and normal shape.
Aorta and cava: no injuries.
Bladder: little full, regular walls. No collections or adenopathies are observed.
Conclusions: Study without specific pathological images.
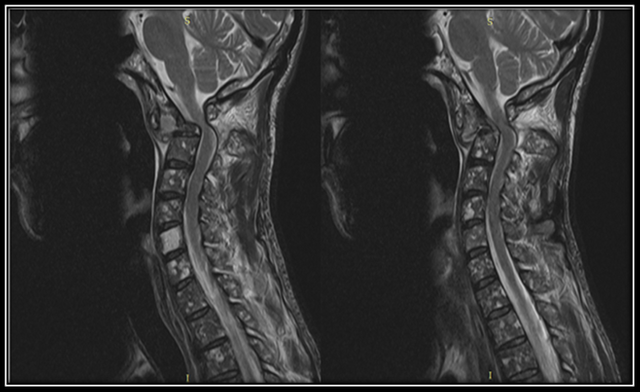
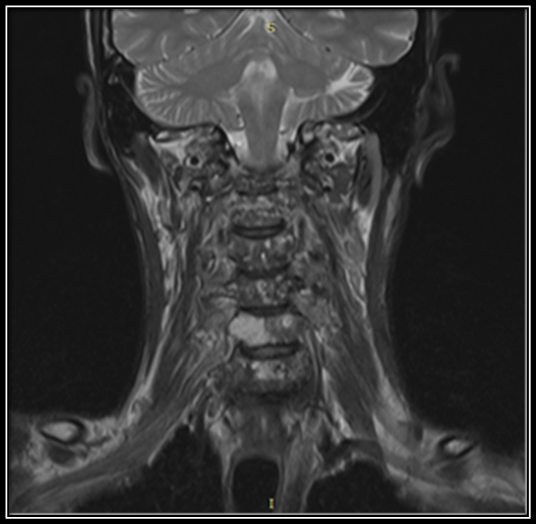
Resonance of Cervical Column
Positive findings:
Resonance images below
Without contrast
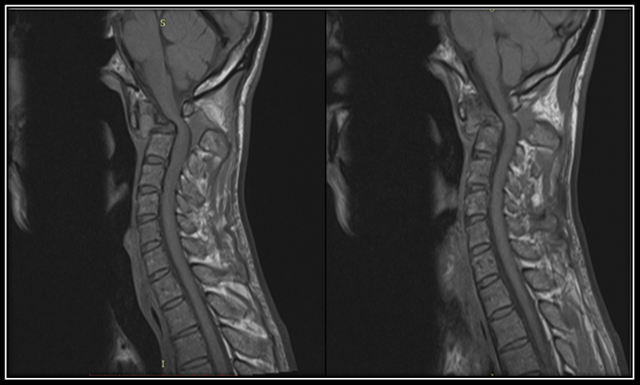
With contrast
Intrahospital evolution
During its in-hospital evolution the patient receives steroids with partial improvement of dysphagia and dysphonia, was evaluated by Neurosurgery service evidencing protrusion of C4-C5 and narrowing of the medullary canal in C1, indicate to rule out neoplasia. On the part of Neurology quadriparesis IV / IV, with hyperreflexia and some sensory alterations, in neuroimaging evidences medullar compression in C1-C2 important anterior and posterior, and the vertebral bodies with lytic lesions, suggesting evaluation by Hemato-oncology, diminishing steroids progressively. By hematology they decide to perform a bone marrow aspirate (pending the result).
Discussion
The spine is a complex and sophisticated bone structure, which allows us to maintain balance and stability of the entire human skeleton, and in addition to it, allows through them to run a series of nerves, and neuronal structures, which will allow us to fulfill multiple functions such as movement, sensitivity, touch among others.
This complex column is divided into several portions; cervical, thoracic and lumbar spine, sacrum and coccyx.
In relation to the case presented, the affected portion is the cervical column, consisting of 7 vertebral bodies, one above the others joined by complex joint systems, the first two being called; vertebra atlas (cervical 1) and axis (cervical 2), which allow the movements of the neck.
In our patient, the cervical vertebra 2 or also called Axis was clearly affected, where what was striking was the increase in volume in the posterior region of the neck not associated with infectious processes, together with a series of symptoms such as dysphagia, weight loss, muscle strength It should be noted that all this clinical picture was not a product or subsequent to a traumatic event whose kinematics of the trauma could explain the patient's clinical symptoms.
Now, we have a patient with a pathological fracture, originated spontaneously, with no known pathological history, which is why multiple complementary studies were requested among them:
Indirect tumor markers (laboratory tests), with LDH and alkaline phosphatase slightly elevated, rest of the paraclinic within normal limits.
Ultrasound with no finding or tumor lesions is found in search of a primary lesion that explains bone involvement, since both radiographs and cervical spine tomography show lytic lesions, which are metastatic lesions that affect the bone. weakens, and predisposes to pathological fractures at any time.
There is no primary neoplastic lesion that explains these lesions, including the prostate being one of the most frequent organs affected and infiltrating bone, it is unscathed. In search of a primary lesion that explains our clinical picture, it is assessed by haemato-oncology, where a sample of bone marrow is taken, and immunohistochemistry, in search of a hematological neoplasm that has gone unnoticed.
We must be clear, that our patient is in age group and sex for multiple myeloma hematological diseases despite the fact that the blood lines are not affected and nothing is evidenced in peripheral blood smears, which is why it is decided to take of bone marrow.
Currently our patient is stable, waiting for results to start oncological treatment.
NOTE: all content is the product of a real clinical case.
The images are property of anaestrada12.
Sources of support in the publication

steemSTEM is a project of the chain of blocks that supports the scientific content in different areas of science. If you want to know more about this wonderful project you can join the server in discord
This article will be published at https://www.steemstem.io/
I hope you enjoyed my content.
Hey there, very nice article. Would you be so kind to tell us where the X-ray image are from?
Best
Chapper
Hi how are you? @Chappetron, the images are resonances made in the hospital where I work, the pathology is a real case of a patient who attended about 6 months ago. I forgot to mention it at the end of my publication, thank you very much for your appreciation.
It's awesome that you can share photos like these. Your posts really help us understand the detective work that health professionals go through in diagnosing patients and the xrays are key to your descriptions.
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @utopian-io.
If you appreciate the work we are doing, then consider supporting our witness stem.witness. Additional witness support to the curie witness and utopian-io witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Thanks for having added @steemstem as a beneficiary to your post. This granted you a stronger support from SteemSTEM.
Thanks for having used the steemstem.io app. You got a stronger support!
Hi @anaestrada12!
Your post was upvoted by Utopian.io in cooperation with @steemstem - supporting knowledge, innovation and technological advancement on the Steem Blockchain.
Contribute to Open Source with utopian.io
Learn how to contribute on our website and join the new open source economy.
Want to chat? Join the Utopian Community on Discord https://discord.gg/h52nFrV
Hi @anaestrada12! I'm not a doctor, just a person. I read this with alarm. The poor patient. I imagined the distress, unexplained symptoms. Inability to swallow. How is the patient dealing with the uncertainty? And how does treatment proceed without clarity of diagnosis?
I hope you let us know how things work out for this patient. To me, it's not x-rays...it's a person. I'm sure that is true for you, also.