Disease and EKG
It is very useful for the evaluation of acute chest pain, palpitations, syncope, and acute dyspnea, and it is the gold standard for the diagnosis of cardiac arrhythmias, conduction disturbances, preexcitation syndromes, channelopathies, and some aspects of acute ischemic heart disease.
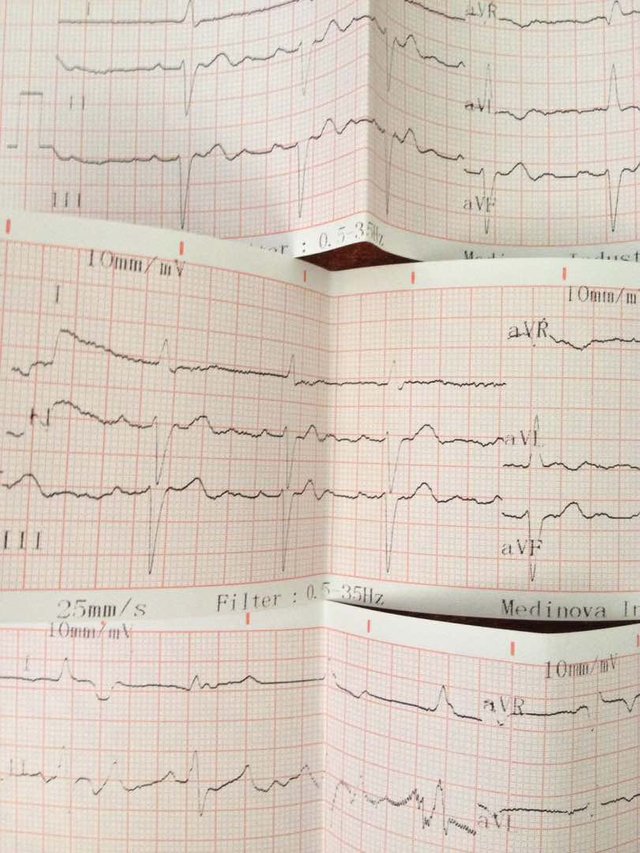
The ECG is a linear recording of the electrical activity of the heart that repeats over time, taken from outside the body by surface electrodes. For each cardiac cycle, different successive morphologies are recorded: atrial depolarization (P wave); ventricular depolarization, called the QRS complex; and ventricular repolarization (T wave). Occasionally, other waves, such as U waves, may be recorded.
When a microelectrode is placed outside and another inside a myocardial cell, a transmembrane diastolic potential, is recorded, which is stable in contractile cells andascendant in pacemaker cells. Then, if is stimulated properly the contractile cell, the monophasic curve called the transmembrane action potential is recorded, which corresponds to the depolarization and repolarization of the cell.
Diabetes frequently causes repolarization alterations. It has been demonstrated that these are more common in patients with coronary heart disease with type 2 diabetes than in patients with coronary heart disease without diabetes.
The most remarkable ECG alterations in electrolyte imbalance are caused by changes in serum potassium levels. In hypocalcemia, the QT may be prolonged at the expense of the ST segment, and in hypercalcemia, the QT may be short.Hypothermia produces typical ECG change the most frequent being baseline irregularities, slow heart rate, prolongation of the PR and QT intervals, and most typically, slurring of the final part of the QRS complex, called the J or Osborne wave.
Alcohol, even when ingested occasionally by healthy subjects, may produce transient repolarization alterations. Chronic alcoholics, particularly those with heart disease, may have persistent repolarization alterations, showing T waves taller than normal or, more characteristically, a low-voltage, bimodal, or slightly negative T wave. Dilated cardiomyopathy may also be present. However, it has been demonstrated that alcohol can trigger different arrhythmias (particularly premature atrial and ventricular impulses, which may disappear with abstinence). Small quantities of alcohol may be protective against IHD, but larger quantities are harmful.
In trained athletes, the ECG is often altered, which suggests chamber enlargement. Occasionally, there are prominent repolarization alterations that cannot be explained by myocardial ischemia. However, as already stated, athletes who experienced sudden death, in whom either hypertrophic cardiomyopathy or coronary heart disease were found on necropsy, often had these striking patterns. Echocardiography detects the presence of LVE and RVE, and in some cases, magnetic resonance imaging is useful.
-----------------------------------------------------------------------------------------------------------------------------------
All this research and images are from my authority.
Your article has encouraged me to start doing electrocardiography at my clinic, it's of great clinical value.
Thank you very much and really nice that this post encouraged you to do that, wish you implement it at your clinic.