INFANT AND YOUNG CHILD FEEDING(BREASTFEEDING)..
Breast milk meets all of an infant's nutritional requirements for the first 6 months of life and is superior to any breast milk substitute.it counters several benefit on both infant and mother, the most important of which is its protective effect against infections such as gastrointestinal and respiratory infections in the infant. Hence the recommendation by WHO and the National Policy on Breastfeeding that children be exclusively breastfed for the first 6 months of life.

Adequate nutrition during infancy and early childhood is fundamental to the development of a child's full potential. It is well recognized that the period from birth to 2 years of age is a "critical window" for the promotion of optimal growth, health, and behavioral development. The consequences of poor nutrition, in terms of both foods and feeding behavior’s, during the first 2 years of life include significant illnesses, delayed mental and physical development and death. Malnutrition is known to predispose infants to the recurrence and severity of diarrhea and acute respiratory infections (ARI), among diseases.
In the long term, early nutritional deficits are linked to impairments in intellectual performance, work capacity reproductive outcomes, and overall health during adolescence and adulthood. Poor breastfeeding practices are linked to all the above, as well as increased fertility and cancers in the mother. Adequate maternal nutrition during pregnancy and lactation are essential for proper breastfeeding.
During pregnancy and lactation, all women need additional food, a varied diet and micronutrient supplement. These ensure that the woman's body reserves are not used up thereby leaving her weakened and unable to meet the optimal demands of breastfeeding. Some of the increased nutrient requirements protect maternal health, while other affect birth outcome and infant health. If the requirement are not met, the consequences can be serious for women and their infants' energy intake. It is important therefore that girls and women action adequate energy intake and a diversified diet throughout their life cycle.
Studies have indicated a high prevalence of malnutrition. Among under-five children, for example, the rate of stunting was 41percent, wasting 14percent, and underweight 23percent,(NDHS,2008).Globally,60percent of children who die from all causes have underlying malnutrition(lancet 2003).the causes of malnutrition are many and complex. Inappropriate breastfeeding and complementary feeding practices coupled with high rates of infectious diseases are the major immediate causes of malnutrition during the first 2years of life. The rate of exclusive breastfeeding for 6months is still very low and has been reported to be 13percent (NDHS, 2008)
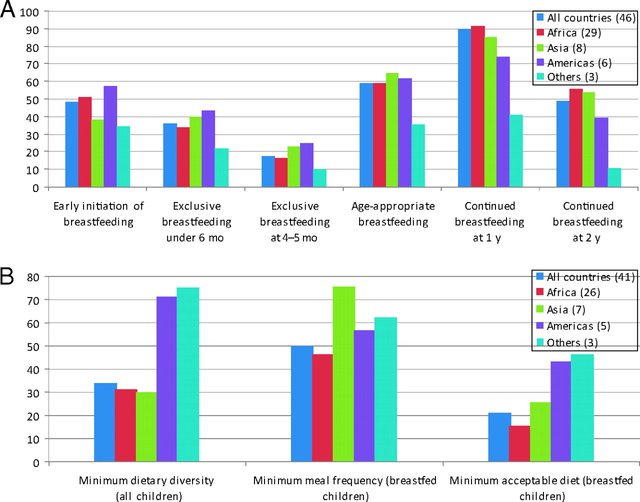
Efforts such as the active baby-friendly hospital initiative (BFHI), training of health professionals in breastfeeding support, and improved hospital practices for the minority of deliveries that are hospital-based could have been responsible for the progress in exclusive breastfeeding recorded in the 1990s. However, this appears not to have translated into overall improved infant feeding practices in the recent time. The unnecessary introduction of water and other fluids reduces intake of breast milk and energy, absorption of iron, and transfer of immune factors from breastfeeding and increases exposure to infectious agents. The majority of children are also not breastfed throughout the second year of life. Without doubt, breastfeeding is recognized as the best feeding option for infants because of its nutritive, protective, psychological and economic values. It should therefore be ordinarily encouraged and supported by all.
The expanding HIV and AIDS epidemic and the prospects of MTCT through breastfeeding did little to sustain the substantial grans of BFHI in the 1990s.Between 1999 and 2008,m the rate of exclusive breastfeeding declined from 17 percent to 13percent(NDHS,2003 & 2008)with attendant negative impact on child survival.
The 2010 WHO guidelines noted the ARV prophylaxis given to the mother and/or baby can effectively block MTCT of HIV though breastfeeding. This new development gave impetus to renewed global drive to promote exclusive breastfeeding for all in facts as an invaluable intervention to improve child survival.
The antenatal clinic sore-prevalence of HIV increased from 4.4percent in 2005 to 4.6percent by the year 2008.The number of people living with the virus is 2.95 million (NDHS, 2008).Consequently, most pregnant women are either HIV negative or do not know their HIV status. Thus protection promotion and support of breastfeeding are extremely important in order not to lose the gains made in child survival during the past few years.
(PMTCT) GUIDELINESS
*The goal of all PMTCT interventions is HIV free-survival of HIV exposed infants and not just prevention of HIV infection in infant;
All mothers including HIV-infected mother should exclusively breastfeed their infants for the first 6months of life and introduce complementary food at 6months.However, HIV-infected mother should continue breastfeeding until 12months while mothers who are HIV-negative should continue breastfeeding up to two years and beyond.
Improved complementary feeding of all infant, and especially those born to Hiv-infected mothers, should be promoted and where possible, supported.
The federal ministry of health will continue to provide antiretroviral drug interventions to reduce the risk of hiv
Transmission through breastfeeding and strongly recommends that all mothers, including those known to be HIV-infected should breastfeed their infants.HIV-infected mother should be assessed to determine if they need lifelong antiretroviral therapy (according to who recommendations) and if so, then to start as early as possible (after presentation to ANC/HIV diagnosis). If HIV-infected mothers do not reduce the risk of HIV transmission should be started and provided until one week after the end at all breastfeeding.
FEEDING MESSAGES FOR CHILDREN AGE: 6 MONTH AND ABOVE
FREQUENCY
*Increase frequency of complementary feeding as the child grows older using a combination of meals and snack while maintaining frequents breastfeeding.
*Feed complementary foods 2-3 times per day.
AMOUNT
*Increase the amount of food as the child grows, putting more on the plate and feeding snacks between meals.
*Introduce ‘finger foods'(snacks that can be eaten by children by themselves) at about 8months of age.
DENSITY
*Gradually increase food consistency and add variety as the child grow older, according to the child's requirements and abilities.
UTILIZATION of food sources
*Give vitamin A-rich foods with fats to increase absorption and give citrus (e.g. oranges, tangerines) with iron to increase absorption.
SAFE
*Wash hands with soap and water before preparing food and before feeding the child
*Keep the food covered in a clean, covered place and re hart before offering to the child.
*Don't give left-over food to the child the next dsy.
*Diversify the child's meal to improve to quality and micronutrient intake by including fruit, vegetables, fortified foods, and/or animal products.
*Feed fruit and vegetables daily, especially those rich in vitamin A (e.g pawpaw, mango, dark green leafy vegetables, and carrot)and vitamins.
*Feed meat, poultry, fish or eggs daily or as often as possible.
*Ensure iron-rich foods or iron supplementation in these months.
*Use fortified foods such as iodized salt, vitamin A, and iron enriched foods.
*Provide meals with adequate fat content.
*When animal products are not available, enrich local staple foods with groundnuts, palm oil, and crayfish.
*Avoid giving drink with low nutrients value and anti-nutrient factors such as tea, coffee, and sugary drinks.
*Control the amount of juice offered so as to avoid displacing more nutrient-rich foods.
*Avoid adding artificial colors, hot spices, and flavors to foods.
*Continue regular growth, monitoring and promotion routine immunization.
*Continue regular use of long-lasting insecticide-treated nets.
PREAMBLE
These recommendation are based in the following
*The provisions of the code of marketing of breast milk substitutes, which were translated into a law which incorporated most aspects of the code and for which a national authority was established in the federal ministry of health (FMOH)
*The global strategy on infant and young child feeding endorsed by world health assembly (WHA),resolution 54.27 of May 2002 which affirm that all innocent goals are to be implemented(Guidelines on HIV and infant feeding (2010).
AGE GROUPINGS
The grouping of infants and young children used in the document for purposes of appropriate feeding recommendations is as follows.
*Birth-6 months
*6 months-8 months
*9 months-11 months
*12 months-24 months
*24 months-60 months
This classification is important because appropriate child feeding requirements are age specific and also defined within very narrow age range, especially for children under 12 months of age.
ESTABLISH PROPER POSITIONING AND ATTACHMENT
*The infant should be held close to the mother, facing the breast, with the infant's ear, should, and hip in a straight line (belly to belly).
*The infant's mouth should open wide just before attaching so that the nipple and as much of the areola as possible are in the mouth. If the infant is properly attached, the lips are curled outward, with the tongue over the lower gum.
BREASFEED EXCLUSIVELY FOR BIRTH TO 6 M0NTHS OF AGE
*Breastfeed only, or when necessary feed expressed breast milk .Give no pre-lacteal feeds and no water or other food or liquids or local herbs. However, drop or syrups consisting of vitamins, mineral supplements, or medicines can be given when prescribed.
*Mother should drink water when thirsty and breastfeed to satisfy the infant's need for water (breast milk contains enough water for the infant) even in dry condition.
PRACTICE FREQUENT, ON DAMAND BREASTFEEDING DAY AND NIGHT
*For best results, feed the infant from one breast until it is empty before offering the second breast. The infant should pass urine at least 5-7times a day and produce stool regularly if in fact of breast milk is sufficient.
*The in fact should breastfed every 2-3 hours day and night (8-12 times in 24hours) or more frequently especially during the first few monthly’s of life.
*To encourage effective sucking and prevent the introduction of contaminants, don’t use feeding bottles or pacifier (dummies or artificial test).If a mother has to miss a breastfeed, she can maintain her supply by expressing milk (EBM) can be fed by cup at a later time. Expressed breast milk is safe for up to 8 hours at room temperature. If refrigerated, it is safe for 24 hours with stable power supply.
*Ensure a home visit or other contacts 3-7days after delivery by a health worker or a trained community support group member to assess and support breastfeeding.
ABBREVIATIONS AND ACRONYMS
ACC-administrative committee on coordination of the United Nations
NDHS-national demographic and health survey
PMTCT-prevention of mother-to-child transmission of hiv
SSS- salt and sugar solution
WHO- world health organization
WHA-world health assembly
{kind=link}
{kind=link}
{kind=link}
In India it is suggested that you should breatfeed your child till 6 months and other than that you should not give anything not even water.
This is top top quality research and writing, well source and well written. I hope this can be trending
Wow
i will keep milking my mom...lol.
Nice this post has hit a spot on the Steve top5 post congrates, the list will be out in few hours.....
CONGRATULATIONS
🎉🎉
Thank you for this interesting article with proper research and statistics. I wish I was able to breastfeed my kids after 3 weeks exclusively, but not one of them gained weight. Even with adjusting my diet, drinking supplements to boost my milk etc. So yes, it is fair to say I envy those women who was able to breastfeed for longer.