Examination of the Cranial nerves
I hope the below may be useful in aiding both medical students and junior medical staff revise examination of the cranial nerves: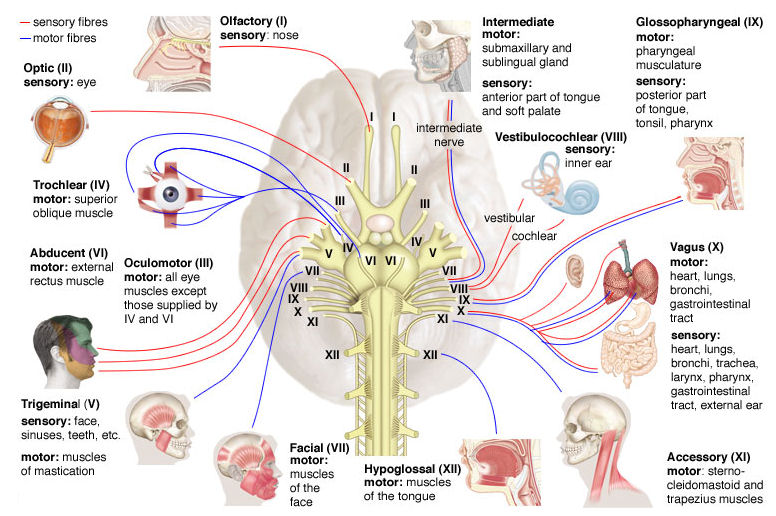
I (olfactory)
- Test the ability of each nostril to distinguish common smells (coffee, lemon), ask if smell has changed recently.
II (optic)
- Acuity - Snellen chart one eye at a time
- Visual fields - finger wiggle, comparing against own fields of vision
- Pupils - size, shape, symmetry, reaction to light (direct and consensual), and test for accommodation if reaction to light is poor.
- Swinging light test - looking for relative afferent pupillary defect.
- Ishihara colour test plate - tests for colour blindness
- Fundoscopy - offer fundoscopy
III (oculomotor), IV (trochlear) & VI (abducens)
- 3rd n. palsy - Ptosis, large pupil, eye down and out.
- 4th n. palsy - Diplopia on looking down and in (often noticed on descending stairs) - head tilting compensates for this.
- 6th n. palsy - Horizontal diplopia on looking out.
- Tested using the H-test, with extended reach looking for Nystagmus
V (trigeminal)
- Involved in sensory supply to the face and motor supply to the muscles of mastication.
- The 3 sensory branches include: ophthalmic, maxillary & mandibular and are tested for sensation to light and deep touch in 3 areas (around the jawline, on the cheek, and on the forehead).
- May also offer to elicit the corneal reflex
-Testing of the motor supply - ask the patient to clench their teeth feeling both the temporalis & masseter mm. - May also offer to elicit the jaw jerk reflex
- N.B. a trigeminal motor palsy will result in the jaw deviating to the side of the lesion when asking the patient to open their mouth.
VII (facial)
- Supplies the motor function to the muscles of facial expression. It is tested by asking the patient to:
-Wrinkle their forehead/ raise eyebrows
-Close eyes against resistance
-Puff out their cheeks
-Grin revealing their teeth
Facial n lesions cause droop and weakness. As the forehead has bilateral representation in the brain only the lower 2/3rds is affected in UMN lesions → forehead sparing. In LMN lesions all of one side of the face will be affected.
N.B. taste can be tested (rarely) as the facial nerve has some involvement in the anterior 2/3rd of tongue via the chorda tympani.
VIII (vestibulocochlear)
- Provides innervation to the hearing apparatus of the ear.
- General hearing - tested by asking the pt to repeat numbers whispered into the ear whilst blocking the other via rubbing the tragus.
- Sensory and conductive hearing loss - can be tested by using the Rinne (tuning fork on mastoid and then next to the ear - air conduction should sound loudest), or the Weber test (tuning fork placed on forehead and patient asked if it sounds louder in either ear).
IX (glossopharyngeal) & X (vagus)
- The glossopharyngeal n supplies sensory supply to the palate and can be tested by eliciting the gag reflex
- The vagus n supplies motor function to the pharynx, and can be tested by asking the patient to say “aah”. Close attention should be paid to the uvula, as vagus n lesions lead to uvula deviation away from the side of the lesion.
XI (spinal accessory)
- Provides motor supply to the sternocleidomastoid and trapezius muscles. It can be tested by asking the patient to shrug their shoulder (trapezius), and turn their head against resistance (SCM).
XII (hypoglossal)
- Provides the motor supply to the muscles of the tongue.
- Ask the patient to stick out their tongue and look for any evidence of fasciculations or wasting.
- The tongue deviates towards the side of a lesion.