Shocking, Shameful Negligence at the Heart of Modern Medicine Which May Be Killing You Draft v0.3
Introduction
This article is a quick explanation of the extremely serious problems I've discovered at the heart of modern medicine, specifically in the field of haematology, which mean that doctors are failing to diagnose and treat simple nutritional deficiencies. These simple deficiencies of folate, B12 and iron may be ruining your health and slowly killing you. They result in a negative feedback loop of gradually worsening metabolism, due to lack of oxygen, which will eventually cause chronic ill-heath and premature death.
I've already written an article about how doctors failed for decades to diagnose the fact that I was suffering from hypoxia due to mercury poisoning from dental amalgam[1]. There were clear, telltale signs in my full/complete blood count, i.e. over the top-of-the-range parameters such as MCH and MCHC, which should have led doctors to the correct diagnosis with a little, logical thought but unfortunately didn't. This was despite me suggesting to them what might be wrong, fairly accurately as it transpires, from as early as 2008. I saw the top consultant haaematologists in the UK, specialising in macrocytosis and B12 deficiency, but they failed to diagnose me. Worse, they also refused to help me by giving me a trial of folic acid or increasing the frequency of the vitamin B12 injections I was already prescribed for life as a result of chronic vitamin B12 deficiency of unknown aetiology. One told me that the issue with my MCH was a matter for research and intimated that he might put me forward to be included in such research but that didn't transpire. I was left seriously ill and deteriorating. Thankfully, however, after many years of my own research, I solved this problem myself[1].
Hypoxia is a well-known condition discussed in detail in the haematology textbooks used by medical schools in the UK and I presume most countries around the world. Quite why doctors are unable to recognise it when they see it, I have no idea. It was certainly totally illogical in my case as it is characterised by an increase in the amount of haemoglobin in red blood cells which I clearly had. Now, hopefully, thanks to my work, they ought to be able to diagnose and treat what I suspect are huge numbers of people, many with chronic neurological conditions, currently suffering and dying unnecessarily due to mercury poisoning and potentially poisoning by other heavy metals.
Not only have I made what, I think most people would agree, is an important discovery regarding mercury poisoning, but I've also made what I believe is an even more important discovery which exposes the fundamental failure of doctors and scientists to understand the mean corpuscular volume (MCV) and how it elucidates the folate, B12 and iron deficiencies many suffer from better, in some cases, than the many other tests available. Unfortunately, this totally inexplicable failure to understand, fully, this most fundamental of all the tests doctors do, in my opinion, ultimately renders much of what doctors and scientists think they know about medicine obsolete or redundant. Quite simply, they are going to have to go back to the drawing board and redo much of the scientific literature. There's nothing else for it. They simply haven't been considering the effects of hypoxia and undiagnosed macrocytosis and microcytosis on the metabolisms of patients and how this impacts apparently unrelated conditions. If they haven't been diagnosing and treating these simple nutritional properly then they have no idea what conditions may be completely cured or at least ameliorated by doing so. I think that the implications of this are quite staggering. It will seriously erode the credibility of doctors and scientists worldwide resulting in their advice and recommendations no longer being as trustworthy to patients particuarly when, as they have recently, extended their purview into all areas of our lives. On the say-so of doctors and scientists, we've had our lives completely turned upside which may have been completely unnecessary had they properly diagnosed and treated us for our nutritional deficiencies resulting in far healthier immune systems able to cope with cold and other viruses with ease.
I've been trying to get help from various doctors and scientists to back me up in this matter for at least 12 months. In fact, I've been trying to get help with this for more than two years but, unfortunately, it's not been forthcoming despite some of them saying that they would help me. I've been trying to write a far more detailed document to explain things but, as luck would have it, in the course of researching for this document, I discovered that the NHS appears to have accepted what I told the MHRA despite the apparent denials of their expert witness in haematology and included it in a document published by NICE[2]. This has given me a helpful shortcut to get this information out so that it can begin to help patients, not just in the UK but, around the world.
Background
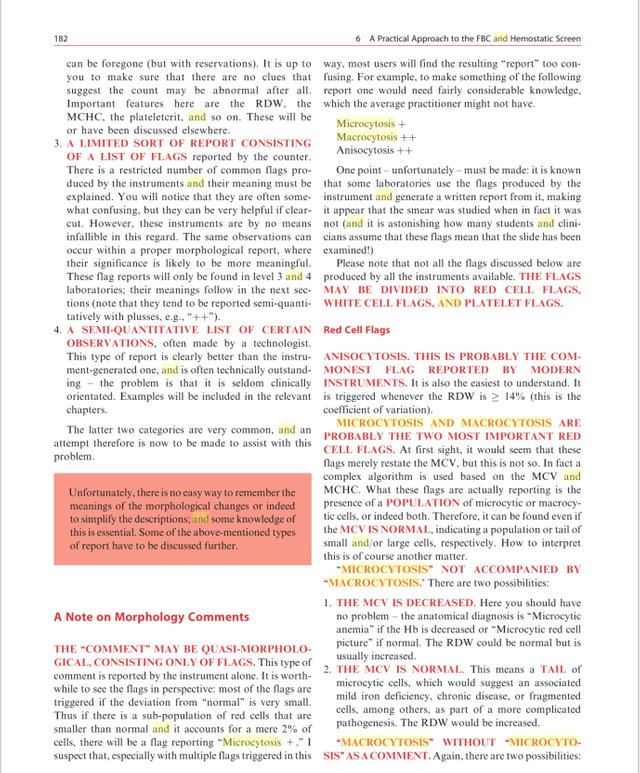
In February 2021, I wrote a detailed email to the Medicines and Healthcare products Regulatory Agency (MHRA) regarding the Sysmex XE-2100 Differential Analyser - Automated Cell Counter because it was failing to flag up a situation whereby a patient had both a macrocytosis (folate and/or B12 deficiencies) and a microcytosis (iron deficiency) but the mean corpuscular volume (MCV) was normal and the mean corpuscular haemoglobin (MCH) was over the top of the range. Normally, the MCV and MCH should track one another, i.e. if the MCV was normal the MCH should be normal, if raised, both should be raised. When the MCV is normal and the MCH is over the top-of-the-range, logically, this should indicate a possible combined macrocytosis and microcytosis. Automated Cell Counters like the Sysmex XE-2100 should be able to flag up the presence of macrocytosis and microcytosis even when the MCV is normal, see page 182[3]. Unfortunately, despite obtaining the full print out from this analyser, there were no flags indicating the presence of macrocytosis or microcytosis anywhere. The failure of the analyser to flag up the microcytosis, which I believe it should have, was what I was complaining about. It seemed to be a fault with the analyser and potentially in the training given to the biomedical scientists who operate it. MHRA is responsible for monitoring such training too.
It took a very long time, until 5th November 2021, to receive a response to my complaint. Apparently they had brought in an expert witness in haematology to address my concerns. Unfortunately, rather than revert to me and ask for more information, their expert and experts from Sysmex, rejected my complaint with some poorly argued, illogical responses. On 20th December 2021, I wrote an extensive rebuttal containing much more information but this was just ignored. I showed clearly using the red cell histogram (RCH) from my full blood count that there was a microcytic tail which categorically demonstrated that I had an iron deficiency which was never diagnosed by any of my doctors and now the MHRA and Sysmex experts had also failed to do so too. It seems that more recent Sysmex analysers have flags for MicroR and MacroR, i.e. to flag up the presence of microcytic and macrocytic red blood cell populations[4], but this really shouldn't be necessary when the red cell histogram, as in my case, clearly shows a microcytic tail. This should've been picked up by the biomedical scientist dealing with my test and flagged up to the doctor. Unfortunately, however, as a result of an encounter with a biomedical scientist to whom I showed my cell histograms, they seem to have a rather cavalier attitude towards such microcytic tails and seem to think that they're insignificant which they clearly are not to the health of the patient.
A few weeks later, in a discussion with a friend, we came to the conclusion that the MCV was simply the average of the MCV of the macrocytosis and the MCV of microcytosis. In other words, if there was a macrocytosis and microcytosis then it was possible for a MCV indicating a macrocytosis, i.e. a MCV > 100 fL, to be reduced into the normal range by the MCV of the microcytosis as in my case. The corollary of this is that a microcytosis could be increased into the normal range by a macrocytosis. Essentially speaking this should be obvious and, indeed, it's explained in at least the Diagnostic Haematology[3] textbook on page 182 in as many words. Clearly, it's unacceptable that something which is already an established fact like this should be misunderstood by any doctor or biomedical scientist because they should understand the full/complete blood count inside out as it's the most basic tool in their diagnostic toolbox.
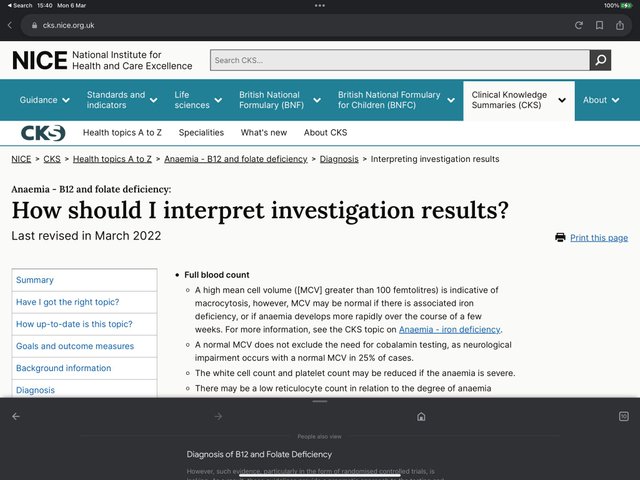
For example, the National Institute for Health and Care Excellence (NICE), Clinical Knowledge Summaries (CKS), for Anaemia - B12 and folate deficiency[2] states, "A normal MCV does not exclude the need for cobalamin testing, as neurological impairment occurs with a normal MCV in 25% of cases." If 25% of patients actually have macrocytosis due to a B12 deficiency which is then reduced into the normal range by an undiagnosed iron deficiency then it's hardly surprising. All doctors should know that this is what's happening. There really can't be any excuse for them not knowing this. This is the exact situation I've found myself in and endured severe, chronic ill-health for decades as a result. What use are these sophisticated automated blood analysers if the information they produce is either ignored or, worse, not understood by those operating them. It's clearly not logical that a specialised branch of science has been created to train scientists in the operation of these machines and they're subsequently found to be incapable of understanding something which should be as basic as this.
Many of my friends and family currently find themselves in the situation where they have low MCV which is clearly due to an iron deficiency but not severe enough to be diagnosed as a microcytosis, i.e. a MCV < 80 fL. However, the actual situation is that they do, in fact, have a microcytosis that's severe enough to be diagnosed as such but their MCV is being increased into the normal range by an undiagnosed macrocytosis. Tragically, they simply never have their folate and B12 deficiencies diagnosed and treated and suffer horrifically being treated with iron infusions which simply can't work because their livers have deteriorated so much due to the impaired DNA synthesis caused by the folate and B12 deficiencies that they can no longer hold the ferritin they need. I explain the mechanisms by which I believe this happens below.
It really is astonishing that biomedical scientists and doctors are unable to cope with the relatively simple logic required to understand the above such that they are unable to diagnose and treat these simple deficiencies properly. They are reduced to something that's akin to guess work as can be seen in the NICE Guidelines[2] and whether or not a patient gets the treatment they need is down to the willingness of the doctor to acknowledge that they have B12 or folate deficiencies simply by virtue of their symptoms, even though the serum and other blood tests apparently don't show them. I can't understand how a committee of experts such as that which has been discussing these NICE Guidelines for years, apparently had no idea about this scenario. It really ought to have been clearly understood from the beginning but they clearly don't fully understand it even now.
In February 2022, I sent this information to doctors and scientists I thought would help me get this information out to the public and their fellow doctors so that the huge number of people struggling to get the right treatment for their folate, B12 and iron deficiencies could finally do so. Unfortunately, help has not been forthcoming thus far. Sadly they appear to be afraid to expose something which will cause such severe problems for their profession even if it would be to the benefit of patients, ease suffering and save huge numbers of lives.
Useful Revelation in The NICE Guidelines
Fortunately, however, because I was researching for the article I was writing, I noticed that, much to my astonishment, it now says in the NICE Guidelines[2], which were last revised in March 2022, that, " ... MCV may be normal if there is an associated iron deficiency ... " This is, of course, exactly what I've been saying. Unfortunately, it doesn't mention the corollary, i.e. that MCV may be normal if there's an associated folate and B12 deficiency increasing it, i.e. when there is an iron deficiency.
The mere fact that this is in the NICE Guidelines confirms what I've been saying without having to write a detailed document and hoping that people believe me despite not having the backing of any doctors or scientists.
I will, however, eventually finish my document pulling together the evidence from haematology textbooks and scientific papers showing that this is a huge problem at the heart of haematology which is leaving millions in the UK alone suffering and ultimately dying unnecessarily simply because doctors can't diagnose and treat simple nutritional deficiencies properly despite having all the tools necessary to do so at hand.
Useful Revelation in Haematology Textbook
I also noticed during the course of my research for my new article that the information I'm trying to get across, which appears to be a revelation to most doctors and scientists, is actually elucidated on page 182 of a haematology textbook I purchased several years ago[3].
It explains that MCV can be normal when there is either a macrocytosis, microcytosis or both. Apparently there is a complex algorithm featuring the MCV and MCHC that can flag up their presence and set what are described by the author as the two most important red cell flags MACROCYTOSIS and MICROCYTOSIS. Why on earth it doesn't appear to be present in the output from the Sysmex XE-2100 I don't know. Perhaps its processor isn't fast enough or something equally mundane. Ultimately, of course, it wouldn't be necessary if the tell-tale, obvious signs of this problem were spotted by well-trained, biomedical scientists or doctors. In my case the microcytic tail in the red cell histogram and red flagged red cell indices MCH, MCHC, etc.
An even bigger mystery, of course, is why the experts from Sysmex who advised the MHRA, didn't mention this. They really ought to know of this algorithm and which of their analysers supports it. The extensive training that they provide for biomedical scientists who operate their analysers really ought to ensure that they understand that this is a known scenario and to be on the look out for it. It would certainly have saved me a great deal of suffering, not to mention my career, had they been able to do so. I think that this model of blood analyser has been in use in my local hospital almost since it became available in the early 2000s.
How to Find Out if You Have a Problem
Everyone really needs to visit their doctor, have a full/complete blood count along with other tests such as serum B12, serum folate, serum iron, Active B12, Methylmalanoic Acid (MMA), homocysteine, etc., to find out whether or not their chronic health conditions may be caused by these deficiencies. It's possible to have these deficiencies and be asymptomatic too so, really, everyone should have these tests done periodically. It's also useful to ask for your cell histograms which can help in diagnosis.
The red cell histogram (RCH), in particular, is useful because it should have the reference normal curve superimposed on it with a MCV of 96 fL. Essentially speaking, if your MCV isn't 96 fL, it may be abnormal and you might have these deficiencies which need to be diagnosed and treated[5].
If your MCV is less than 96 fL, you should consider the possibility that you have an iron deficiency and if it's over 96 fL, you should consider the possibility that you have folate and/or B12 deficiencies. However, you must also consider the possibility that if you have a normal MCV > 96 fL it may indicate that there are folate and/or B12 deficiencies and there may be an iron deficiency reducing its severity. The corollary, as already mentioned, is that you must also consider the possibilty that if you have a normal MCV < 96 fL, you have an iron deficiency but may also have folate and/or B12 deficiencies increasing your MCV into the normal range. I believe that huge numbers of people are currently in these situations and suffering extreme symptoms which doctors simply don't believe because their MCVs and serum blood tests are normal. I can scarcely believe that this situation has persisted for decades without someone coming along before me to straighten it all out.
Basic Mechanisms Causing Macrocytosis, Microcytosis, Hypoxia and Anaemia
Here I describe the basic mechanisms by which mercury poisoning from dental amalgam caused my hypoxia and led to the deficiencies which resulted in folate, B12 and iron deficiencies. I think that many other toxins operate using many of the same mechanisms.
Since the Covid-19 spike protein also causes hypoxia, I think that this information is probably very relevant to those who've been harmed by that. I know that many of them are still suffering with no real diagnosis or treatment and I suspect that they are suffering from these deficiencies which aren't being diagnosed or treated. The spike protein is known to be toxic and causes inflammation likely leading to folate and B12 deficiencies as described below. Since it's a virus that can replicate tremendously throughout the body, I suspect that it can put people into the methylfolate trap very rapidly indeed.
- Mercury vapour, chemical formula Hg0, is released from the dental amalgam filling during and after chewing.
- The mercury vapour is inhaled, enters red blood cells (RBC) via the lungs where it binds with haemoglobin thereby preventing it binding with oxygen.
- Mercury also enters the gut where it displaces copper which is necessary for the absorption of iron thereby causing iron deficiency.
- Mercury is antibacterial and so may kill off certain important bacteria in the gut leading to an inability to absorb certain nutrients from food thereby causing deficiencies.
- Mercury, being extremely toxic, damages cells and causes inflammation which increases the body's need to perform DNA synthesis and repair. This involves a process known as methylation which also, as a result, increases demand for vitamins such as folate and B12 in particular.
- Once oxygen levels have been reduced sufficiently, the body may react by effectively adapting to altitude and begin creating RBC containing more haemoglobin than normal in an attempt to increase oxygen levels.
- The process of increasing the amount of haemoglobin in RBC in order to increase oxygen levels may not be very successful because, as a result of folate and B12 deficiencies, the RBC may be macrocytic or microcytic which means that they are unable to diffuse enough oxygen due to their reduced surface area, plus they are unable to deform in order to pass through capillaries meaning oxygen doesn't reach vital tissues.
- I've noticed that some people seem to increase the number of RBC rather than increase the amount of haemoglobin.
- Some people seem to be unable to adapt to the low oxygen levels and will eventually become anaemic rather than hypoxic.
- Those who do become hypoxic, without treatment for their deficiencies, may eventually become anaemic as they become more and more folate, B12 and iron deficient.
- As the ability to synthesis and repair DNA becomes more and more impaired, the body's ability to maintain and repair itself decreases resulting in normal wear and tear such as that to the liver not being repaired. Eventually, the liver becomes so damaged that it is no longer able to store ferritin which is released in the bloodstream where it may confuse doctors into believing that there is no iron deficiency. However, since ferritin must be released from the liver as transferrin in order to be used by the organs, this results in iron deficiency. In the case of mercury poisoning, it's compounded by the fact that iron absorption is impaired because of the iron deficiency caused by the copper deficiency created in the gut as a result of it being displaced by the mercury.
- As the ability to synthesise DNA deteriorates along with the metabolism, the immune system is adversely affected. In my case, I was neutropenic and suffered from many severe skin infections as well as allergic rhinitis.
- Clearly, as the iron deficiency worsens, the body is unable to produce as much haemoglobin which ultimately, without treatment, leads to anaemia.
- As accessible oxygen levels fall, the metabolism is reduced, eventually leading to epigenetic changes resulting in the body falling into the methylfolate trap.
- When in the methylfolate trap various conditions occur such as neurological conditions, severe inflammation and impaired immune function due to an inability to synthesis and repair DNA. A full discussion is outside the scope of this document but I intend to write in more detail about this in due course.
- Low levels of oxygen in the blood may affect the health of the lining of the gut adversely affecting the diversity of the microbiome, resulting in malabsorption of nutrients further exacerbating nutritional deficiencies.
- In my case, the copper deficiency eventually led to me being diagnosed with possible myelodysplasia. Copper deficiency is known to mimic myelodysplasia.
Based on the above, it's possible to have folate and B12 deficiencies without an iron deficiency but, eventually, you are likely to have all three due to the impaired DNA synthesis and repair damaging the liver. Doctors should take the red cell indices and cell histograms into account in order to determine which deficiencies are present. Also, in the case of those with clear signs of folate, B12 and iron deficiencies, an elevated or even just normal haemoglobin level or MCH may still indicate hypoxia. I suspect that many people suffering with conditions such as "Constant Air Hunger" are actually hypoxic but doctors are missing it, leaving them to suffer terribly. I was so adapted to my situation that I was barely aware of the fact that I had what others referred to as "the sighs", i.e. I had take a deep breath as though I were sighing in order to get more oxygen. It was something I did without realising.
Duty of Care
Doctors in the UK have what's known as a duty of care towards their patients. It may be called other things in other countries. However, essentially speaking, the primary duty of all doctors is for the care and safety of patients. Therefore, once made aware of this situation as outlined in this document, doctors must address the shortcomings of their knowledge and immediately take remedial actions to diagnose and treat patients properly.
I have successfully treated myself and recovered once. Unfortunately, however, my GPs refused to cooperate with me when I asked for a prescrition for folic acid and I fell into remission. I was unaware at the time that the underlying problem was mercury poisoning and so reducing the levels of nutrients I was taking would inevitably result in me getting sick again. I'm still trying to recover to this day although, hopefully, I'm on the way now. I have only been aware that mercury poisoning caused my problems for approximately two years.
I would like to write a document outlining what I've done to recover but I have quite a lot on my plate and I'm not physically able to do much work at the moment.
Medical Negligence Case
I have been trying to find someone with the means to help pay for my medical negligence case in order to bring these issues to the public attention. There have been several occasions where my medical negligence case was supposed to be underway but various problems prevented it. On the last occasion, for some reason, it seemed to be a condition that I accept that I had a non-existent, adverse, mental health condition in order for it to go ahead. Naturally I wasn't prepared to accept that. Unfortunately, when you are dependent upon things like conditional fee agreements and after the event insurance, it seems that you're effectively forced to accept whatever you're offered even when it constitutes a cover up of a massive public health problem such as mercury poisoning from dental amalgam. If the medical and legal establishments wish to cover up the fact that they've been poisoning millions of people with mercury from dental amalgam, then you have to accept that if you want to be compensated for what was done to you. My conscience simply won't allow me to do that.
So, if there is an individual or group of individuals interested in funding a medical negligence case which will transform medicine into the service its patients deserve, whether it wants to or not, please get in touch with me at jimherd at protonmail dot com.
As far as I'm concerned, given what I've uncovered, the medical profession have been abusing their positions as guardians of our health. It's clear to me that we need to democratise the types of information I've uncovered so that it can no longer be withheld from us leaving us suffering and dying anymore. It doesn't matter whether or not this situation is the result of logical failure or intent. It simply can't be allowed to persist.
Unfortunately, my circumstances won't allow me to rely on public donations so I really do need to find somoeone or a group that can fund my case. I do not want to be in a situation where I'm forced to settle my case and allow the medical profession to continue mistreating us the way it has.
Conclusion
It's unfortunate that I've uncovered such serious failings in medicine, particularly haematology, but I think most people would agree that it's important that this information is available to the general public, doctors and scientists so that urgent steps can be taken to begin to resolve the situation. People are suffering and dying every day because they have these easily diagnosed and treated nutritional deficiencies which are often caused by toxins from medical and dental treatments, i.e. are no fault of the patients. It really is a Bloody Scandal that this situation has been allowed to endure for so long without being exposed. It's no surprise, however, given my own experiences of being gaslit, threatened, assaulted, battered and generally mistreated by the medical system. Medical professionals who spot such problems with medical care are also threatened and abused too but I think things have gone so far that they really should have no choice but to stand up and be counted.
Needless to say medical professionals are going to be unhappy at being humiliated by a patient solving these problems and exposing them to the public. Scientists are going to be angry that their work has been shown to be inadequate because it didn't take into account the metabolisms and epigenetic states of the subjects of their experiments. Wealthy people who've made fortunes out of producing medicines which patients will no longer need will be less than happy at the loss of revenue. They all should know that there have been several opportunities for the NHS and others to settle my case with me long before I knew what I know now. I'm extremely glad that they made it impossible for me to do a deal with them because it forced me to continue my research and ulitmately solve these problems which they would much rather I hadn't. That's what I call karma in action.
The Establishment have been well aware of what I've been up to and have gone to extreme lengths to try to stop me getting the help I need to expose these issues and save lives. They haven't stopped me and they won't stop me. I just hope that the help I need to deal with these matters will be forthcoming very soon from people who don't want to let them get away with what they've been doing to us.
References
- Shocking Reasons Why Doctors Are Ruining Lives By Failing to Diagnose Mercury Poisoning Second Draft.
- National Institute for Health and Care Excellence (NICE), Clinical Knowledge Summaries (CKS) Anaemia - B12 and folate deficiency.
(https://cks.nice.org.uk/topics/anaemia-b12-folate-deficiency/)
- Diagnostic Haematology, Dr Norman Beck, Springer-Verlag London Limited 2009.
(https://www.google.co.uk/books/edition/Diagnostic_Hematology/ZVP-jwEACAAJ?hl=en)
- The microcytic (MicroR) and macrocytic (MacroR) red blood cell populations ([https://www.sysmex-europe.com/academy/knowledge-centre/sysmex-parameters/micrormacror.html](https://www.sysmex-europe.com/academy/knowledge-centre/sysmex-parameters/micrormacror.html))
- The Red Cell Histogram and The Dimorphic Red Cell Population ([https://academic.oup.com/labmed/article/42/5/300/2505011](https://academic.oup.com/labmed/article/42/5/300/2505011))