Campus Ed: Urinary Incontinence{10% delegation to Campus Connect}
Greetings! Steemians, Today, I'll be talking on condition commonly seen in women, Most women come down with it as a result of child birth etc.. Its the weakness of the pelcvic floor muscle . It's called Urinary Incontinence . Urinary Incontinence (UI) is a prevalent problem that is frequently untreated. Prevalence estimates differ based on the population investigated, the measurement period (daily or weekly), and the severity instruments utilized. Although it is believed that 50 percent of adult women and 3 percent to 11 percent of adult males are affected, only 25 percent to 61 percent of those women seek treatment.This could be due to embarrassment, a lack of understanding about treatment alternatives, or a notion that urine incontinence is a natural part of growing older.
Urinary Incontinence
• Urinary incontinence (symptom): An uncontrollable loss of Urine
• While knowing which kind of urine incontinence to treat can help, an individual may experience symptoms from more than one classification.
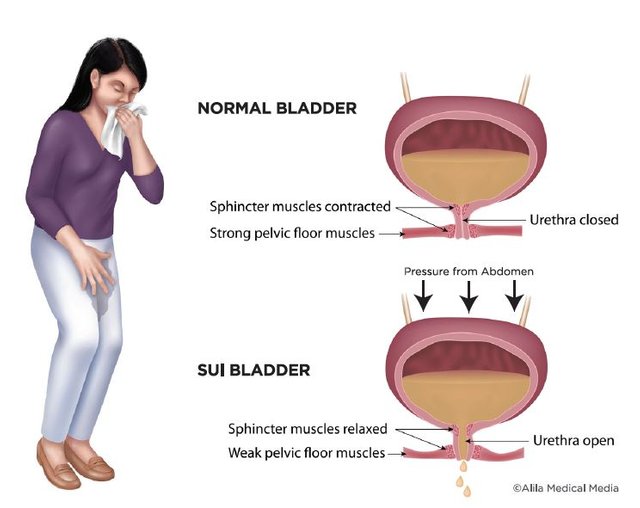
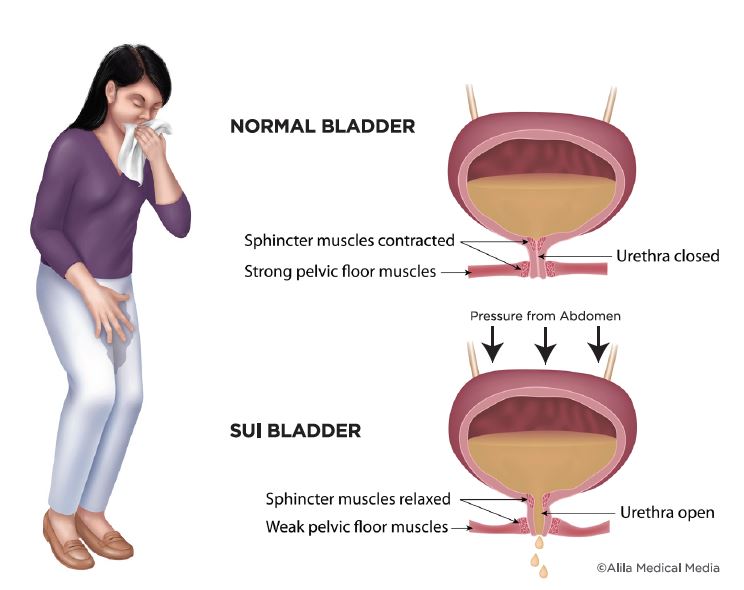
Pelvic Floor Anatomy Is Clinically Relevant
- The pelvic floor is made up of muscles, ligaments, and fascial structures that work together to support the pelvic organs and give compressive forces to the urethra under elevated intra-abdominal pressure.
- The levator ani, striated urogenital sphincter, external anal sphincter, ischiocavernosus, and bulbospongiosus are all parts of this complex.
- The urethra, vagina, and rectum all flow through the pelvic floor and are encircled by the pelvic floor muscles.
- The pelvic floor muscles must contract to give support as intra-abdominal pressure rises. The urethra, anus, and vagina close when the pelvic floor muscles flex.
- The contraction is necessary to prevent involuntary urine or rectal contents loss.
- To void, the pelvic floor muscles must also relax.
Epidemiology
Urinary incontinence is a widespread disease that affects both men and women of all nations and races. As previously said, determining the global prevalence is challenging due to variances in definitions, population polled, survey style, response rate, age, gender, health care access and efficacy, and other factors.
Etiology
- vaginal birth,
- post-partum,
- obesity,
- chronic cough,
- chronic heavy lifting,
- constipation.
- bladder abnormalities,
- increased or altered bladder microbiota are all possible causes.
- Delirium
Risk Factor
• Obesity • Parity • Delivery Mode • Family History • Other: • Childhood nocturnal enuresis • Estrogen depletion
Note: Individuals can have many types of incontinence. For example, stress and/or urge incontinence may be "masked" by an overactive bladder (frequenting the restroom frequently to avoid leaking).
Types of Urinary Incontinence
Overactive bladder: This can be caused by neuropathic pain, infection (e.g., urinary tract infection), weak pelvic floor muscles, diuretics, drugs, or being overweight
Incontinence due to stress: It manifests clinically as involuntary pee loss caused by coughing, sneezing, laughing, or other physical actions that raise intra-abdominal pressure.
• In the absence of a detrusor contraction, SUI is characterized as urine loss accompanied by an increase in intraabdominal pressure.
• The most prevalent cause in women is urethral hypermobility, or substantial displacement of the urethra and bladder neck during exertion, in the absence of a detrusor spasm or an over-distended bladder (pressure)
SUI can also be induced by an intrinsic urethral sphincter deficiency, which can occur in patients with myelomeningocele, epispadias, or pelvic denervation due to congenital sphincter weakness.
• It can develop after a prostatectomy, trauma, radiation therapy, or a lesion in the sacral cord.
• Intrinsic Sphincter Deficiency (ISD) in women is frequently linked to repeated incontinence surgical procedures, as well as hypoestrogenism, age, or both.
• The urethral sphincter in ISD is unable to provide adequate resistance to keep pee in the bladder, especially under stressful situations.
• ISD patients frequently leak continually.
Urinary incontinence Due to Urge
Urinary incontinence accompanied with a strong desire to discharge (urgency). It's frequently linked to involuntary detrusor contractions or detrusor instability on urodynamic examination (DI). Although DI is linked to neurologic problems, it can also affect people who appear to be healthy.
• UI can be caused by DI's unrestrained bladder contractions, which can occur with or without signs of urgency. It can also produce urge incontinence without causing incontinence. The DI is known as detrusor hyperreflexia (DH) when a causal neurologic lesion is identified.
• DH has been linked to stroke.
• Suprasacral spinal cord lesions/multiple sclerosis: Detrusor sphincter dyssynergia (DSD) (inappropriate external sphincter contraction with detrusor contraction) is a common complication of DH.
• Detrusor hyperactivity with impaired bladder contractility (DHIC) is frequent in the elderly — involuntary detrusor contractions, but they must strain to empty their bladders entirely or partially.
• DHICs typically have UI and a high PVR, but they may also have blockage, stress incontinence, or overflow incontinence.
Overflow Incontinence is the involuntary loss of urine caused by bladder overdistension. It might show as dribbling that is regular or persistent, as well as urge or stress incontinence symptoms. An underactive or acontractile detrusor, as well as a bladder outlet or urethral obstruction, can result in overdistension and overflow.
• Drugs, neurologic disorders such as diabetic neuropathy, low spinal cord injury, or major pelvic surgery can cause the bladder to be underactive or acontractile.
Clinical Significance
• Urinary Frequency
• Urinary Urgency
• Nocturia
• Prolapse
Treatment
The kind of incontinence, its severity, and the underlying reason all influence the treatment of urinary incontinence. It's possible that a combination of treatments will be required.

{kind=link}
{kind=link}
- Bladder training is a technique for delaying urinating when you feel the urge to go. You might begin by delaying urination for 10 minutes whenever you feel the desire.
- Double voiding can help you learn to empty your bladder entirely and avoid incontinence due to overflow.
- Instead of waiting until you need to go, schedule restroom trips every two to four hours.
- To regain bladder control, you must regulate your fluid and food.
- Exercises for the pelvic floor muscles, such as Kegal Exercises
- Medications like Anticholinergics, Mirabegron (Myrbetriq), and Alpha blockers can be used .
In conclusion Urinary Incontinence is can cured when managed by right professional and the importance of a physiotherapist should not be overlooked when managing the underline conditions.
Thanks for reading,
@stellaheart, Thanks for sharing with us on @campusconnect , Continue sharing your quality contents with us here we love and appreciate your effort ,Thanks
REMARKS;
Thank you for contributing to #LearnWithSteem theme. This post has been upvoted by @reminiscence01 using @steemcurator09 account. We encourage you to keep publishing quality and original content in the Steemit ecosystem to earn support for your content.
Regards,
Team #Sevengers