STAY ENLIGHTENED - COLORECTAL CANCER IS REAL
Hello steemit !
I promised to play my part through my contributions to the steemit community. Am a final year medic and I feel I owe my world education about common health challenges in our world today.
This article highlights colon-rectal cancer from the doctor's view . I hope this answers some questions .
WHY COLO-RECTAL CARCINOMA ?
Am sure you're wondering but I have taken time out to under because I have an Uncle who's being managed for Colo-Rectal cancer and it's really been a burden psychologically and financially. So I wish to educate my world so we can be enlightened on the scourge that is Colo-Rectal cancer.
We'll review this pathology under the various headlines .
- Introduction
- Epidemiology
- Aetiology
- Clinical Presentation
- Investigation
- Therapeutic Interventions
- Preventive
- Conclusion/Important notes
Brief introduction
What is Colo-Rectal Cancer ?
Colon cancer is a type of cancer that begins in the large intestine (colon). The colon is the final part of the digestive tract. It's quite common and presents as a very lethal condition
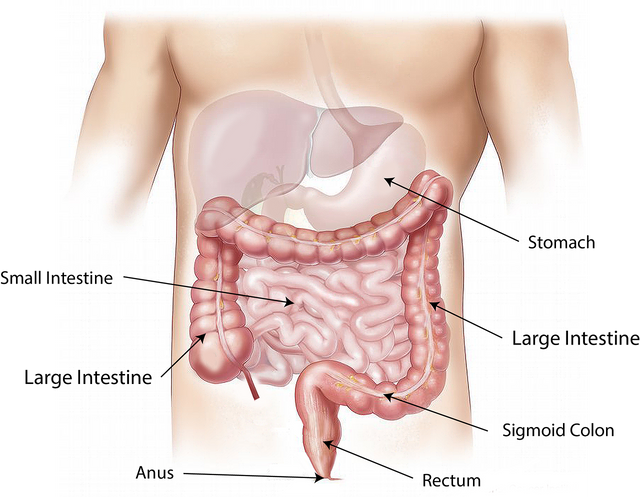
It's anatomy comprises the ascending colon, transverse colon and descending colon and sigmoid colon. These form part of the digestive system that terminates as the rectum.
Source
A graphical illustration of the terminal aspect of the gut including the small and large intestine.
EPIDEMIOLOGY
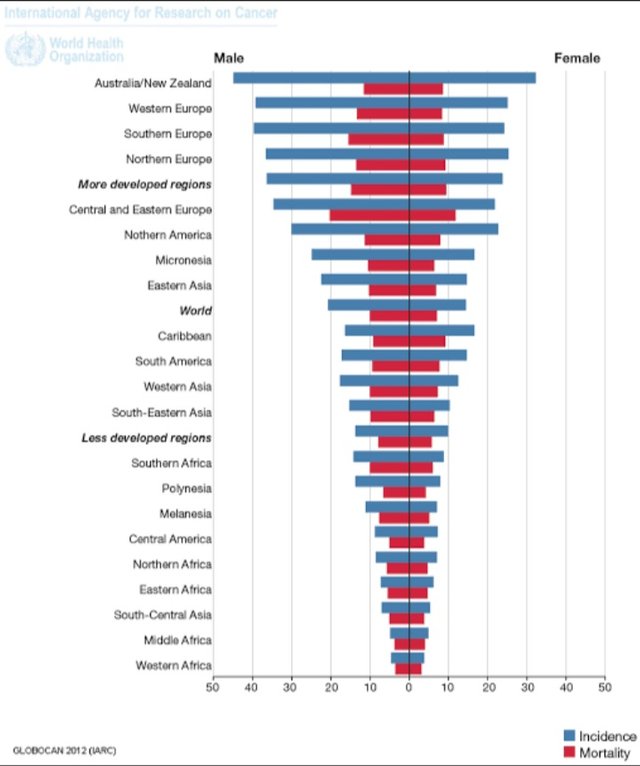
The epidemiology would be reviewed based on incidence and mortality
Incidence
According to GLOBOCAN 2018 data, cancer of the colon is the fourth most incident cancer in the world, while cancer of the rectum is the eighth most incident. Together, CRCs are the third most commonly diagnosed form of cancer globally, comprising 11% of all cancer diagnoses.
About 1,096,000 new cases of colon cancer were estimated to be diagnosed in 2018, while about 704,000 new cases of rectal cancer were expected. Together, these comprise 1.8 million new cases of CRC. CRC is the most diagnosed cancer among men in 10 of the 191 countries worldwide. No country has CRC as the most diagnosed cancer among women.
Mortality
The CRC was the second most deadly cancer worldwide, with about 881,000 deaths estimated for 2018. Colon cancer is the fifth most deadly cancer with 551,000 deaths projected for 2018, comprising 5.8% of all cancer deaths. Meanwhile, rectal cancer is the 10th most deadly, with 310,000 deaths, which constitutes 3.2% of all cancer deaths. The cumulative risk, at age 0 to 74 years, of dying from colon cancer is 0.66% among men and 0.44% among women. The same risk for rectal cancer is 0.46% among men and 0.26% among women. Age-standardised (world) mortality rates per 100,000 of CRC in both sexes is 8.9
AETIOLOGY
Generally cancers don't have a specific cause but are found to have close associations. These are risk factors and those associated with increased risk of colo-rectal cancer include :
BETHESDA CRITERIA
Below are the Revised Bethesda Guidelines for testing colorectal tumors for microsatellite instability (MSI).
- Colorectal or uterine cancer diagnosed in a patient how is less than 50 years of age
- Presence of synchronous, metachronous colorectal, or other HNPCC-associated tumors, regardless of age.
- Colorectal cancer with the MSI-H histology diagnosed in a patient who is less than 60 years of age.
- Colorectal cancer diagnosed in one or more first-degree relatives with an HNPCC-related tumor, with one of the cancers being diagnosed under age 50 years.
- Colorectal cancer diagnosed in two or more first- or second-degree relatives with HNPCC-related tumors, regardless of age.
Genetics
A personal history of colorectal cancer or polyps. If you've already had colon cancer or noncancerous colon polyps, you have a greater risk of colon cancer in the future.
Family history of colon cancer.
You're more likely to develop colon cancer if you have a blood relative who has had the disease. If more than one family member has colon cancer or rectal cancer, your risk is even greater.
Race
African-American race. African-Americans have a greater risk of colon cancer than do people of other races.
Age
Older age. Colon cancer can be diagnosed at any age, but a majority of people with colon cancer are older than 50. The rates of colon cancer in people younger than 50 have been increasing, but doctors aren't sure why.
Diet
Low-fiber, high-fat diet. Colon cancer and rectal cancer may be associated with a typical Western diet, which is low in fiber and high in fat and calories. Research in this area has had mixed results. Some studies have found an increased risk of colon cancer in people who eat diets high in red meat and processed meat.
Lifestyle/Health Consciousness
A sedentary lifestyle. People who are inactive are more likely to develop colon cancer. Getting regular physical activity may reduce your risk of colon cancer.
Obesity.
People who are obese have an increased risk of colon cancer and an increased risk of dying of colon cancer when compared with people considered normal weight.
Smoking.
People who smoke may have an increased risk of colon cancer.
Alcohol.
Heavy use of alcohol increases your risk of colon cancer.
Iatrogenic (Caused by attempts by health workers at therapy)
Radiation therapy for cancer. Radiation therapy directed at the abdomen to treat previous cancers increases the risk of colon cancer.
Other Pathologies
Inflammatory intestinal conditions.
Chronic inflammatory diseases of the colon, such as ulcerative colitis and Crohn's disease, can increase your risk of colon cancer.
Inherited syndromes
that increase colon cancer risk. Some gene mutations passed through generations of your family can increase your risk of colon cancer significantly. Only a small percentage of colon cancers are linked to inherited genes. The most common inherited syndromes that increase colon cancer risk are familial adenomatous polyposis (FAP) and Lynch syndrome, which is also known as hereditary nonpolyposis colorectal cancer (HNPCC).
Diabetes.
People with diabetes or insulin resistance have an increased risk of colon cancer.
CLINICAL PRESENTATION
Symptoms of colon cancer can be looked at systematically
GASTROINTESTINAL TRACT SYMPTOMS
Diarrhoea : This involves passage of watery stools . It could result from the irritation of the bowel lining (mucosa)
Constipation : Difficulty in passing stools due to bowel obstruction
Constipation alternating with diarrhoea :
Bleeding per rectum : Also referred to as Hematochezia. The blood might be frank-red or brownish depending on the source of the bleeder.
Persistent abdominal discomfort, such as cramps, gas or pain probably due to pressure symptoms or an ulceration or perforation.
Tenesmus :A feeling that your bowel doesn't empty completely .
N/B : These symptoms may vary based on the location of the tumor. Tumours in the ascending , transverse and descending colon and rectum present differently a level of clinical knowledge is needed to ascertain the site of the lesion based on presenting symptoms.
GENERAL SYMPTOMS
Weakness or fatigue : could be a pointer to anemia due to an acute or chronic blood loss which could be occult(hidden) or visible.
Unexplained weight loss : this symptoms is usually illicited in cancer patients and patients with ill-managed chronic illnesses.
it's very important to note that many people with colon cancer experience no symptoms in the early stages of the disease. When symptoms appear,they'll likely vary, depending on the cancer's size and location in your large intestine.
Emergency Presentations
In emergency cases , the patient would need immediate resuscitation and possibly an emergency laparotomy.
This presentation include cases of
Acute Intestinal obstruction
this usually presents as
- Excruciating pain
- Distention of the abdominal wall
Peritonitis
Here there could be generalized abdominal pain. This usually occurs due to
- a perforation secondary to a blind-loop obstruction or
- from progressive ulceration of the bowel
Massive Low G.I Bleeding
this could be from a perforation that bleeds through the anus
LABORATORY INVESTIGATIONS
Labs help the doctor make a definite diagnosis and decide the best next course of action. Also some other labs are done to determine the client's preparedness for surgery. This labs are jeered towards avoiding intra-operative complications.
DIAGNOSTIC INVESTIGATIONS
The Gold standard for making diagnosis is Colonoscopy !
Other investigations to determine diagnosis include
Proctoscopy
Double contrast Barium Enema
Endoscopic Ultrasound
Feacal Occult blood
PRE-SURGICAL INVESTIGATIONS
This include tests to stage the pathology and also to determine if the patient is fit for surgery !
Abdominal Computerized Tomography/Magnetic Resonance imaging
Positron emission tomography scan
Liver function tests
Renal function tests
Abdominal and Chest X-rays
THERAPEUTIC APPROACH
In summary there are three modalities for treatment
Surgery
Usually done to resect the tumours
Chemotherapy
Usually given as pre or post-operative medication to manage the cancer
Radiotherapy
The application of these modalities depend on the percularity of the case in view so we might not be able to go into details
PREVENTION
Screening colon cancer
Doctors recommend that people with an average risk of colon cancer consider colon cancer screening around age 50. But people with an increased risk, such as those with a family history of colon cancer, should consider screening sooner.
Talk about your options with your doctor, and together you can decide which tests are appropriate for you.
Lifestyle changes to reduce your risk of colon cancer

You can take steps to reduce your risk of colon cancer by making changes in your everyday life. Take steps to:
Diet
Eat a variety of fruits, vegetables and whole grains. Fruits, vegetables and whole grains contain vitamins, minerals, fiber and antioxidants, which may play a role in cancer prevention. Choose a variety of fruits and vegetables so that you get an array of vitamins and nutrients.
Alcohol
Drink alcohol in moderation, if at all. If you choose to drink alcohol, limit the amount of alcohol you drink to no more than one drink a day for women and two for men.
Tobacco
Stop smoking. Talk to your doctor about ways to quit that may work for you.
Exercises
Exercise most days of the week. Try to get at least 30 minutes of exercise on most days. If you've been inactive, start slowly and build up gradually to 30 minutes. Also, talk to your doctor before starting any exercise program.
Maintain a healthy weight. If you are at a healthy weight, work to maintain your weight by combining a healthy diet with daily exercise. If you need to lose weight, ask your doctor about healthy ways to achieve your goal. Aim to lose weight slowly by increasing the amount of exercise you get and reducing the number of calories you eat.
Colon cancer prevention for people with a high risk
Some medications have been found to reduce the risk of precancerous polyps or colon cancer. For instance, some evidence links a reduced risk of polyps and colon cancer to regular use of aspirin or aspirin-like drugs. But it's not clear what dose and what length of time would be needed to reduce the risk of colon cancer. Taking aspirin daily has some risks, including gastrointestinal bleeding and ulcers.
These options are generally reserved for people with a high risk of colon cancer. There isn't enough evidence to recommend these medications to people who have an average risk of colon cancer.
If you have an increased risk of colon cancer, discuss your risk factors with your doctor to determine whether preventive medications are safe for you.
CONCLUSION
In conclusion, colorectal cancer as the third most common cancer amongst men and women should be talked about more often. Regular screening should be done for at risk individuals.
Keywords :
CRC Colo-Rectal Cancer
HNPCC Hereditary nonpolyposis colorectal cancer
MOST OF THE DETAILED INFO WAS GOTTEN FROM LECTURES GOTTEN DURING MY TIME IN MEDICAL SCHOOL.
REFERENCES
1.Colon cancer[Internet] .Available from: https://www.mayoclinic.org/diseases-conditions/colon-cancer/symptoms-causes/syc-20353669
2.Macrae FA. Colorectal cancer: Epidemiology, risk factors, and protective factors. Uptodate com [ažurirano 9. lipnja 2017. 2016 Jan.
3.Pourhoseingholi MA. Epidemiology and burden of colorectal cancer in Asia-Pacific region: what shall we do now. Transl Gastrointest Cancer. 2014 Oct;3(4):169-73.
4.Rawla P, Sunkara T, Barsouk A. Epidemiology of colorectal cancer: Incidence, mortality, survival, and risk factors. Przegla̜d Gastroenterologiczny. 2019;14(2):89.
5.Ladabaum U, Wang G, Terdiman J, Blanco A, Kuppermann M, Boland CR, Ford J, Elkin E, Phillips KA. Strategies to identify the Lynch syndrome among patients with colorectal cancer: a cost-effectiveness analysis. Annals of internal medicine. 2011 Jul 19;155(2):69-79.