The Physical Location of Depression in the Brain

Depression affects many people. Now, researchers have pinpointed the areas of the brain that correlate with how we experience depression.
The brains of 909 people in China were scanned with an MRI. Half had depression and half didn't (421 to 488). The medial and lateral orbitofrontal cortexes (OFC) responsible for emotion and rewards/punishment operated differently in those who had depression. The lateral OFC activates when we are disappointed, like when an expectation is not met. For people with depression, this area of the brain was more connected to the area for our sense of self and identity, the precuneus.
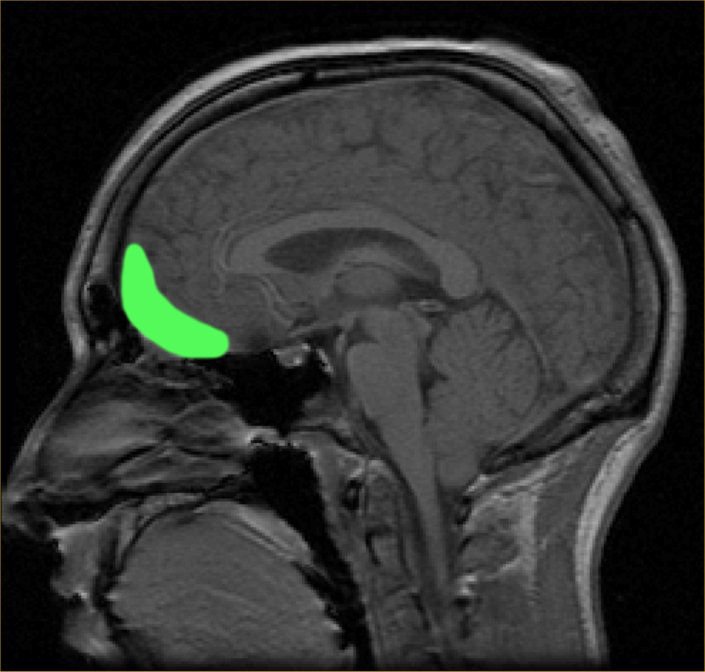
This could explain part of the depression cycle. As expectation are not met, they think they are note valued by others or not worth getting what they thought they would get. They devalue themselves to lower their self-esteem and how they view themselves overall, their self-view, self-image and sense of self. Having the rewards and self-evaluation aspects connected too much leads to a backfire of what we might expect.
Coupled with this, is the finding that the medial OFC is less connected to the memory areas, meaning less recall of positive memories to balance out their perception of the negative happening now.
Researchers hope these finders could lead to specific treatment of the area of the brain required. An additional benefit is that negative thoughts in depressed people is reduced.
I did a post a while back teenage depression being on the rise. Even among adults it's an issue, as over 10% of people will have depression at some point in their lifetime.
I have long suspected that depression is a result of incorrect perfections of reality that produce unmet expectations due to not seeing reality correctly. As such, the root cause of depression is not in the brain, but psychological in consciousness. There is a feedback.
The drugs they want to develop are still only dealing with the secondary layer of how the brain reacts to epigenetic environmental factors affecting how we think, fee and act. Something happened in life that was not necessarily physical, but psychological in life, and this acts as a minor or major trauma to our psychological makeup, our self-view and world-view. And then the brain electro chemical operation is changed as a result. I don't deny some real physical issues that preexist psychological trauma.
@krnel
2016-11-22, 12am
Nice post! I would add that gut health and the mind body connection seems to play a role in helping depression. Lots of clinical drugs have some debatable results and could be hardly better than a placebo. Some of them have some rather nasty long term side effects. I've found focusing on my breath and really watching my diet helpful for me. Also not watching the news has been a help for me recently too.
Yup, mostly psychological true root cause, the brain responds to how we think and feel in addition to creating our ability to think or feel. Placebo demonstrates that the mind can induce states in the body. Breathing, diet, are all changes we can make that don't require drugs that never deal with the psychology in the first place.
Thanks for sharing :)
Interesting as always
This post has been ranked within the top 25 most undervalued posts in the first half of Nov 22. We estimate that this post is undervalued by $8.71 as compared to a scenario in which every voter had an equal say.
See the full rankings and details in The Daily Tribune: Nov 22 - Part I. You can also read about some of our methodology, data analysis and technical details in our initial post.
If you are the author and would prefer not to receive these comments, simply reply "Stop" to this comment.
Listening people saying that a psychological trauma preexist a depression is like listening people saying that epilepsy is diabolical possession. There are several hypothesis around the mechanism of depression, but is a disease had been described since by Hippocrates 2400 years ago. Even in the Bible (1 Samuel 18, 8-10) is described an evil spirit from God came upon Saul" (c.630–540 BC).
Really sad the darkness of mental illness.
In order of the mechanism , some information:
Hypofrontality
One of the most consistent findings in the neuroimaging of depression is decreased cerebral blood flow (CBF) and glucose metabolism in the PFC, particularly the DLPFC. Several studies have found negative correlations between depression severity and frontal metabolism.
yperactivity and electrical stimulation of Cg25
Certainly one of the most exciting findings in neuropsychiatry in recent years has been the identification of Cg25 as a key region in the pathophysiology of depression. Several neuroimaging studies have correlated hyperactivity in this region with depressed mood states and induced sadness in healthy volunteers and depressed patients. Depression severity is correlated with Cg25 hypermetabolism and increased functional connectivity. Spontaneous and treatment-induced remission of symptoms is associated with significantly decreased Cg25 metabolism.
Activity in the ventral anterior PFC correlates positively with depression severity and activity in this region decreases after effective treatment.
A number of studies have demonstrated that activation of the amygdala with concomitant emotional arousal is very quickly followed by activation of the OFC and – in healthy individuals – suppression of the amygdala response. This suppressive function of the vmPFC/OFC is supported by a large body of preclinical data. It is likely that this function is impaired in depression, with the suppressive/repressive action of the vmPFC/OFC being dominated by persistent flurries of limbic arousal.
Amygdala hyperactivity and electrical stimulation of medial temporal lobes
Hyperactivity in the amygdala has been reported in a large number of imaging studies of depression. Amygdala activity has been found to correlate positively with depression severity, to show a sustained response to negative emotional stimuli in depressed patients compared to healthy controls and to decrease in sensitivity to emotional stimuli after successful antidepressant treatment.
Human tractography and functional connectivity analyses support these findings, showing prominent connections between Cg25 and the NAc, amygdala, hypothalamus, OFC and vmPFC [54, 198, 199]. The connections of Cg25 to a number of important visceromotor centres offering profuse projections to the PFC has led to suggestions that Cg25 plays an important modulatory role in cortical functioning. The magnitude of disconnectivity between these structures predicted anxiety scores in a number of individuals. Resting state connectivity between Cg25 and a range of structures including the medial temporal lobes has been found to predict treatment response in depressed patients and a strong correlation was discovered between subjective measures of neuroticism and Cg25 and amygdala activation during the viewing of emotionally provocative images.
Postmortem and MRI studies have found glial loss and volume reductions in the PFC in major depressive disorder (MDD) and bipolar disorder (BPD) as well as extensive losses in Cg25 and proximal paralimbic regions. Unilateral and bilateral volumetric reductions in the medial temporal regions – primarily in the hippocampus, have also been reported in depressed patients, as have reductions in the ventral striatum.
Mourning and melancholia revisited: correspondences between principles of Freudian metapsychology and empirical findings in neuropsychiatry
And I ended it saying "I don't deny some real physical issues that preexist psychological trauma." i.e. there is depression that is preceded by physical issues.
No need for laughable analogies like "Listening people saying that a psychological trauma preexist a depression is like listening people saying that epilepsy is diabolical possession."
It's important because the fact is that we dont know what was first: the neurological changes or the psychological symptoms. Say that a psychological trauma preexist is a falacy. It is a regressing thought because you are doing a distinction between "soul or mind or psuchological traumas" and body. And this dicotomy is from Middle Ages. Depression is a disease: yes, multifactorial, idiopatic, unknown, yes, but a disease, a medical disease. I showed the review of Freud's neuropsychiatry findings just to show that Freud wasn't a neurologist nor a psychiatrist, he was a psychologist with a great sense of intuition but full of fantasmagoric bullshit. It worked in 1917 but now we are in 2016. What was first: the neuroanatomical and functional alterations or the psychological and physical symptoms?
There are not such things as exogenous and endogenous depression, that stigma was abolished in the early eighties.