Infection in the central nervous system. "Neurocysticercosis"
Next I will share a rare medical topic, but over the years, due to deficiencies in hygiene and quality of food processing, especially in underdeveloped countries, has become an emerging disease.
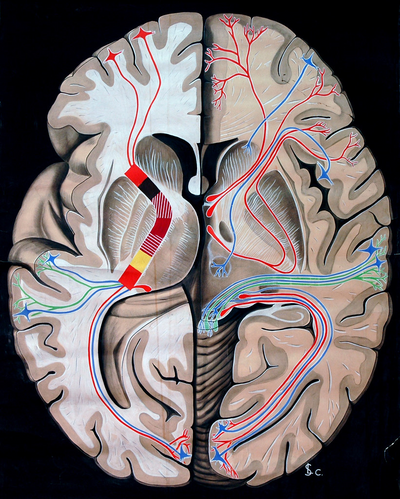
Central nervous system. Public domain source Flickr
Neurocysticercosis is a parasitic infection that affects the central nervous system, a product of the development of small cysts mostly by its agent Taenia solium, which is eaten from contaminated pork meat undercooked or raw, or by the ingestion of food contaminated with feces of a human carrier of this microorganism.
This neuroinfection is usually a pathology with endemic areas in developing countries, reporting the highest incidence rates in countries of Latin America, Asia, Africa and India.
Taenia solium can occur in the body in two forms; intestinal or extraintestinal, affecting the CNS and other tissues such as the skin. The main reservoir of this parasite is the pig, having the man as an accidental host.

This microorganism has characteristics similar to that of a flat worm consisting of a pyriform head (escolex) containing 4 suction cups and a double crown of hooks, which allows it to attach itself to the wall of the intestine of its host. It is followed by the neck and a set of segments called proglottides, which will form the rest of the body.
The parasite has the peculiarity that has both male and female reproductive system, located in each segment of proglottide, so it is considered hemaphrodite, also has no digestive system so their requirements get nutrients digested by the host.
When located in the intestine, this parasite can reach a size between 3 to 5 meters and produce the disease known as Teniasis, which together with Taenia saginata, are species called Solitary Worm.

{kind=link}
This micrograph reveals the morphology of a Taenia solium tapeworm scolex with its four suckers, and two rows of hooks. Public domain source wikipedia commons

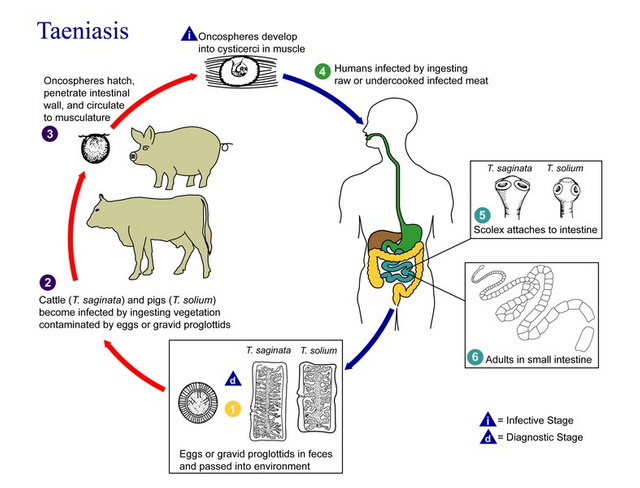
Taenia solium needs both pigs and humans to fulfill its life cycle.
When accidentally ingested by man, the eggs contained it, either by food (raw pork meat) or contaminated water, or in its absence by contamination via anus-hand-mouth.
Under normal conditions, the habitat of this microorganism is the small intestine, where once ingested the eggs by means of undercooked pork meat, they are released into the gastric cavity by the action of stomach acid, where by the action of their scolices they adhere to the wall of the intestine and mature, this takes a period of time of approximately 2 months.
These adult tapeworms have the capacity to produce fertile eggs in their proglottides, which are later released and migrate to the anus. And from there these eggs are released with the feces.
{kind=link}
Life cycle of Taenia solium. Pubñic domain CC BY-SA 3.0. Source wikipedia. Author: CDC/Alexander J. da Silva, PhD/Melanie Moser, Courtesy: Public Health Image Library
These feces contaminated with embryonated eggs have the ability to continue spreading the disease, infected to other human beings, pigs and even an autoinfection, to continue its cycle.
Once they enter the digestive system these eggs release oncosphere that hatch penetrating the wall of the intestinal tract, directing through blood circulation to other tissues such as muscle, skin, liver giving rise to the disease cysticercosis or neurocysticercosis when located in the Central Nervous System.

When this pathogen reaches the CNS via the bloodstream, its cysts lodge in the intraparenchymal zone, having several evolutionary phases and these are:
The first phase or vesicular phase, in an initial phase these viable cysts, constituted by a thin membrane that surrounds the invaginated escolex and translucent liquid, this phase can last years without generating immune response and therefore clinical symptomatology.
Second phase or colloidal phase, there is evidence of an inflammatory response surrounding the cyst with moderate to severe clinical manifestations as a result of important perilesional edema by immune response, characterized by a cysticercus with cloudy liquid accompanied by hyaline degeneration of the escólex.
Third phase or granular nodule phase, where the cyst is composed of fibrotic tissue with a tendency to collapse of its cystic wall.
Finally, the late and inactive calcification phase of the disease, where calcium is added to the fibrotic tissue.
Although neurocysticercosis has a predilection for intraparenchymatous tissue, cases have also been reported outside this area, such as subarachnoid cysts that tend to be large with a lobed appearance (bunches of grapes). These do not have the escólex, and are observed more frequently at the base of the brain or in the fissure of Silvio, where the former is associated with the presence of hydrocephalus and the latter with clinical manifestations of lesions that generate a mass effect such as LOES.
The other location is the intraventricular area, which generates clinical hypertension Endo cranial obstruction or partial block of the aqueducts of drainage of the cerebrospinal fluid.
Inflammation of these cysts can lead to ependymitis and arachnoiditis, which can lead to hydrocephalus, severe perilesional edema that displaces structure or general brain vascular events caused by vasculitis.

This pathology may be asymptomatic in 50% of affected patients. Its symptomatology may in the first instance be non-specific as it is similar to many other diseases of the central nervous system, such as epilepsy.
Depending on its location, clinical signs and symptoms can be observed.

The most frequent place is due to the presence of generalized focal or partial seizures in 80%. When there are more advanced phases accompanied by perilesional edema, it is frequent to observe manifestations of endocranial hypertension.
Bilateral, unilateral headache is a nonspecific symptom that may be present in both intraparenchymatous and extra-parenchymatous localization, which may be accompanied by photophobia, scotomas and even blurred vision, which is why it is important that these patients have a thorough examination to rule out the presence or absence of this parasite at the ocular level as well.
Another symptom observed is focal deficit such as hemiparesis, motor involvement, cerebellar ataxia, and even cognitive impairment.

Here we find cysts lodged in the intraventricular and subarachnoid zones. It is associated with higher mortality and more severe cases with great neurological compromise.
The clinic is specific for hydrocephalus and endocranial hypertension given by headache, nausea, vomiting, arterial hypertension and bradycardia and even the presence of papilledema in the fundus of the eye.
Meningeal syndrome, stiff neck, kernig maneuver and positive brudzinski. It can be accompanied by involvement of cranial pairs, and even paresis or paralysis of extremities.
Less frequently the presence of Bruns Syndrome has been reported: it is characterized by intense headache, vertigo and episodes of loss of consciousness (syncope) which is frequently evidenced when the cysts are located in the 4th ventricle causing obstruction of the cerebrospinal fluid and endocranial hypertension that generate sudden and uncontrolled movements of the head.
It is important to bear in mind that cysts with a subarachnoid location are associated with vasculitis, cerebral infarcts and local or subarachnoid hemorrhages, to such an extent that they may involve cranial pairs.

Striated muscle, subcutaneous tissue; characterized by the presence of palpable and painful nodules.
Optochiasmatic syndrome, due to strangulation of the chiasm secondary to thickened meninges, which generate a decrease in visual acuity. If the extraocular musculature is compromised it can similar paralysis of cranial pairs as the III pair.
Finally, cases of cysticercosis have been reported in the myocardium of post morgue patients, which are capable of generating alterations in the structure of the heart and causing heart failure and conduction alterations.

In general, diagnosis is obtained through complementary studies such as Computerized Axial Tomography or Cranial Magnetic Resonance, which allow us to visualize the cystic images of neurocysticercosis, in addition to certain epidemiological factors, contact with contaminated animals such as pigs, live in endemic areas, travel to these areas, or be carriers of Intestinal Teniasis or extra neural cysticercosis as lesions in muscle or skin.
Also available is a serological study called EITB "Enzyme-linked Inmunoelectrotransfer Blot" which detects specific antibodies to this parasite. Both blood and CSF samples can be taken, with blood samples being more specific and effective.
The definitive diagnosis will be given by the biopsy of these lesions, which allows us to observe under the microscope their histological characteristics, however it is very difficult to take these lesions at the level of the central nervous system.
It is important to perform an assessment of these patients by ophthalmology service in order to elaborate an eye fundus and ocular ultrasound in order to rule out ocular cysts (most frequently located in the retina and vitreous).
Complete with laboratory studies such as hemogram, renal and hepatic function.

This is a 60 year old male patient with a long history of type 2 MD, who refers moderate to strong Holocranean intensity headache that partially subsides with common analgesics, which is later associated with fever quantified at 39.5 ºC, with no predominance of schedule, continues to yield partially with acetaminophen-type antipyretics orally every 4 hours, finally shows the day of admission, loss of muscle strength of left hemicorpus, and neurological impairment given by drowsiness, disorientation, so that prior assessment is admitted.
The patient is admitted to the unit under regular clinical conditions, afebrile, mildly dehydrated, eupneic, tolerating ambient oxygen and decubitus. Isocoric pupils normoreactive to light. ORL without alterations, Neck mobile not painful. Cardiopulmonary thorax symmetrical normo-expansible apex in 6th intercostal space. Audible vesicular murmur without aggregates. Painless depressible soft abdomen, without visceromegaly. Symmetrical extremities without edema. Neurological somnolent with response to painful stimulus, disoriented, without alteration of cranial pairs, left hemiparesis, muscular force II/V, without meningeal signs and unexplored gait due to patient condition.
In view of Neurological compromise, Cerebral Magnetic Resonance is requested where it is evidenced:





In the present study, multiple cystic images of neurocysticercosis, of different sizes and in different phases, vesicular, nodular and calcified, are observed. The large image is that of right occipital parietal location, with important perilesional edema that generates mass effect displacing structures and compressing ventricles.
In view of finding of study of neuroimage, it is valued by the service of neurology, who agree that these lesions are characteristic of neurocysticercosis, in its different stages, being the largest right occipital parieto location in calcified phase but with significant perilesional edema.
Based on what has been described and the clinical manifestations of the patient, treatment with Ev steroids type Dexamethasone 8mg is initiated every 8 hours, with improvement of the neurological state and treatment with Albendazole is indicated at a dose calculated at 20mg/kg of weight per day for 14 days.
Currently our patient is stable receiving the treatment already mentioned waiting to conclude the same to perform neuroimaging control study.
Sources

steemSTEM is a project of the chain of blocks that supports the scientific content in different areas of science. If you want to know more about this wonderful project you can join the server in discord
This article will be published at https://www.steemstem.io/
link
I hope you enjoyed my content.
I'm reflecting on the importance on neurocysticercosis on the behaviour alterations of drug users.
Apart from the contamination issue of street drugs, methamphetamine alters blood-brain barrier allowing a more effective entrance of these pathogens.
It would be interesting if you could share a little of that research you are currently doing, although you probably can not since it could be published in a scientific journal right? @gustavomonraz
null
It would be interesting if you could share a little of that research you are currently doing, although you probably can not since it could be published in a scientific journal right? @gustavomonraz
Congratulations @anaestrada12! You have completed the following achievement on the Steem blockchain and have been rewarded with new badge(s) :
You can view your badges on your Steem Board and compare to others on the Steem Ranking
If you no longer want to receive notifications, reply to this comment with the word
STOPTo support your work, I also upvoted your post!
Vote for @Steemitboard as a witness to get one more award and increased upvotes!
Thank you
You're welcome @anaestrada12
Feel free to support us back: vote for our witness.
You will get one more badge and more powerful upvotes from us on your posts with our next notifications.
Very unique, good to read and interesting again! Thank you! Reminds me on my Zombie article! ;-)
Thank you very much @chappertron your comments are always positive in my publications and you are always following my content. As for your article about the zombie apocalypse, it's a lot of fun to read, full of a lot of interesting information that doesn't stray from reality but makes it a lot of fun. I realized that it was a little underestimated, you received very little support and that's very strange! maybe few people managed to read it, you should consider replicating it, right?
You've got a 100% Steemstem vote, that's all we can offer. Cool that you like the Zombie Post. Be curious what comes next on your Blog. Regards Chapper
Posted using Partiko Android
I was referring to your zombie post which received little support and is very good. I am very happy with the support I have from steemstem I do not complain at all I am very grateful :) @chappertron
@tipu curate
Upvoted 👌
Thank you
@tipu curate :)
Thank you very much
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @minnowbooster.
If you appreciate the work we are doing, then consider supporting our witness @stem.witness. Additional witness support to the curie witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Thanks for having used the steemstem.io app and included @steemstem in the list of beneficiaries of this post. This granted you a stronger support from SteemSTEM.
Thank you very much @steemstem :)
I think I'll stop eating so much pork :P
As long as you cook the meat very well you don't have to worry ;)