FOURIER cholesterol trial: a game changer or evidence that pre-2006 cholesterol research was fraudulent?
We have all been told the story hundreds of times. Cholesterol causes heart disease. High cholesterol, or more precisely high Low-Density Lipoproteins (LDL), is a huge threat to our health, and lowering LDL, either through a diet low in saturated fats and animal products or by using cholesterol-lowering medicine such as statins, or better yet both: a vegan diet supplemented with a high-dosage statin is all that stands between us and prematurely dying from a cardiovascular event. A recent advisory by the American Heart Association underlines this undeniable truth, ones more. LDL is evil, it will kill you, and so will saturated fat as found in butter, beef fat and coconut oil as these fats will raise your LDL levels and high LDL levels will result in massively increased risk with regards to cardiovascular disease. The AHA has reviewed many decades worth of research once again and in its wisdom has come to the conclusion that new insights shared by some brilliant minds in recent years regarding the health risks of LDL have been misguided after all. Well, maybe it has, we have recently seen the 'game changing' results from the FOURIER trail, a two-year, relatively large scale and hugely expensive trial with a new wonder drug that lowers LDL lower than we have ever seen before. And looking at the press coverage of the FOURIER results, it would be hard to not come to the conclusion that LDL lowering is a magical protection against CVD. If next to FOURIER we look at old statin trial data and even older observational studies, all seem to point in the same direction. LDL is out to kill us. But is it?
Mortality as Poisson process
I'm no biochemistry expert, so this post is not going to be a biochemistry post. We are going to look at the published data purely from a data engineering point of view. The main outcomes we are going to be interested in will be cardiovascular events. Roughly, from a data engineering point of view, there are two types of cardiovascular events: fatal events and non-fatal events. In the light of effects of exposure time, both have their issues that can't really be addressed without access to individual event timing info. The issue is that λ might be a function of t. But when we ignore this aspect shared by both types of events another issue remains with including non-fatal events. The problem is that while fatal events happen only once to a given person and therefore are stateless with respect to each other. There is one caveat however. As fatalities deplete the population, even fatal events aren't fully stateless as far as a shrinking population is concerned. For non-fatal events the problem is a bit different. With non-fatal events, in the case of CVD ,individuals who have had an event find themselves at a different level of risk after that event. Individual risk is not stateless and as such the process as a whole can not be assumed to be stateless and as such and could be assumed to mu multi modal. Problem is we can' t know. Picking the right tests is quite impossible in fact without access to raw event data containing enough information to link multiple events to the same person. Much more so for non-fatal than it is for fatal events, even though fatal events have the population depletion effect we just mentioned. If we ignore the possibility of λ might be a function of t for now and assume mortality to be a stateless process determined solely by mortality risk, then mortality becomes what is known as a Poisson process.
We will see later that for FOURIER this assumption is good enough to work with.
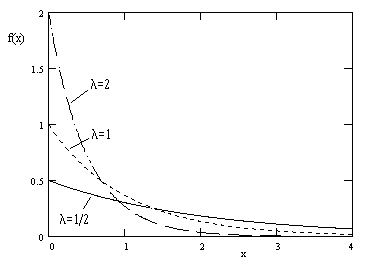
In a Poisson process, the time between two events will be exponentially distributed. The number of events emitted from a Poisson process in a given time span will follow a probability distribution known as a Poisson distribution.
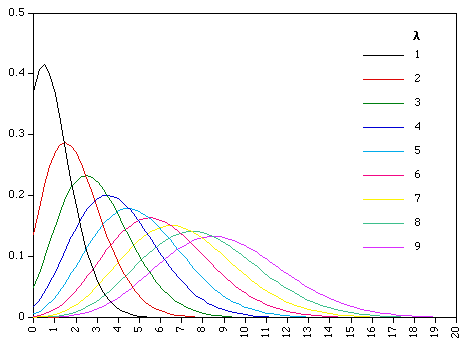
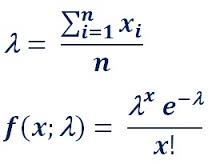
For those of you interested in the math here, the distribution is described by:
Michel de Lorgeril
A few years ago, Michel de Lorgeril made an observation. The results from statin trials used to routinely be very convincing, but since stricter regulations, introduced in 2005/2006, regarding Randomized Controlled Trials (RCTs), the outcomes from such trials all magically seemed to be underwhelming when compared to pre-2006 trial results. Well, this could all be coincidental of-cause, but it still is something to watch out for.
Luckily the FOURIER trial happened. A relatively large trial that had the potential to prove Michel de Lorgeril wrong.
Statins vs LDL lowering
While statins lower LDL, they also do a lot of other things that could potentially be relevant to any potential risk reduction properties. So before we look at FOURIER, a trial using a new non-statin drug from the perspective of Michel de Lorgeril's observation we must note the possibility that even if these results would be in favor of M de Lorgeril's observation, we won't be able to conclusively conclude de Lorgeril right. If however the results of FOURIER strongly conflict de Lorgeril's observation, such outcomes could be strong evidence that these observations indeed were coincidental.
FOURIER: the numbers
Well, if you have been folowing the news, MOST of the figures coming from FOURIER have been rather positive. Amazing lipid profile improvements including massive LDL lowering. Lower non-fatal event rates for a wide range of non-fatal event types, so much good news that the term 'game changer' feels like it is quite appropriate.
Yes, there are some skeptical people making a fuss about the mortality numbers, but at these p-values, these can safely be ignored, right? The study was under-powered for statistical significant mortality figures anyway, and given more time, these would surely follow the trend set by the non-fatal events. With these amazing non-fatal event outcomes we surely have enough evidence to burry de Lorgeril's hypothesis, the LDL hypothesis is back and fully reinstated?
Well.... No! Not so fast. Let us look at that mortality data first. We don't have the raw data, no event timing info that might be useful for non-Poisson arrival time distribution, but we have the CV and all-cause mortality numbers and p-values, and guess what: The p-values published match those of the mortality numbers put into a standard Poisson tests relatively closely. Close enough for us to use a Poisson process as working model:
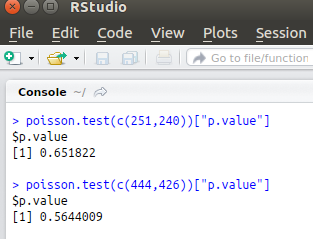

So even though the mortality numbers are even higher for the people treated with the new wonder drug, the people who on average lowered their LDL by a massive 1.6 mmol/l, at these p-values, this is just random noice against our null hypothesis. The null holds, no need to worry about these mortality numbers, hurray, take that Michel.
But wait! What was the null hypothesis for this? The null wasn't: The findings from the pre-2006 trials are all valid. The null was: these two mortality numbers stem from the same Poisson process. And remember, the trial was underpowered to reach any statistical significant outcome against that null anyway. For us to look at what FOURIER could tell us about de Lorgeril's observations, we need to look at some pre-2006 results first and use those as H0.
Primary prevention
While it would be best to use comparable secondary prevention figures as FOURIER was a trial with high-risk secondary prevention patients, a very much enticing study with old data shows us figures that we can easily use for our test. This paper claims a relatively strong risk reduction can be accomplished for primary prevention. It claims that based on a number of old-data studies, a 15% five-year risk reduction for CV mortality per mmol/l LDL reduction. Now that is something we can work with. If we still assume a Poisson process and adjust our FOURIER CV mortality numbers accordingly to the two-year duration and 1.6 mmol/l average reduction, we arrive at a p-value of 0.07 for CV mortality and 0.12 for all-cause mortality. No statistical significance, no, but given the limited power of FOURIER and the fact that this risk reduction was just primary prevention, it is clear we can't dismiss de Lorgeril that easily yet. As such the confidence with what the AHA now proclaims SFA and LDL as causal in CVD should be viewed with quite some reservation.
The literature if filled with findings showing that statins work significantly better for secondary prevention than they do for primary prevention, so taking this into account, while I could find no easy-to-calculate-with quantification of the effect of LDL lowering for secondary prevention in a meta-analysis like this, the probability that such a quantification used to adjust the FOURIER findings would yield significant results is rather high.
Possible explanations
Currently, we can neither reject nor accept de Lorgeril's findings based on FOURIER, combined with old-data meta-analysis above however and papers based on old-data that compare primary and secondary prevention effects of statins, we can conclude that the pieces of the puzzle don't seem to fit. There can be a different explanation for this.
- De Lorgeril is right
- De Lorgeril is wrong in his observation but the positive effect of Statins is not strongly related to its LDL-lowering properties.
- De Lorgeril is wrong and the positive effects of LDL lowering are counteracted by some unknown adverse effect in FOURIER.
Mendelian randomization
Could this spell the fall of the LDL hypothesis? Well, it does weaken it quite a bit, but RCTs are not the only source of evidence. While from a data engineering perspective I believe the evidence for the LDL hypothesis in nowhere near convincing, given de Lorgeril's observations and the failure of FOURIER to proof de Lorgeril wrong in any way, there is one piece of evidence that seems to stand relatively strong in favor for the LDL hypothesis. That piece is Mendelian Randomization. But then, as I'm not a geneticist either, it is quite impossible for me to grasp potential shortcommings of MR.
Conclusion
While there is enticing evidence , in the form of MR results, supporting the hypothesis that LDL may play at least a moderate role in the causality of CVD, there is also strong indications that Michel de Lorgeril's observations regarding other lines of evidence are correct. The most important conclusion: The pieces of the puzzle, from a data engineering perspective, don't fit. Either something is very wrong. Conspiracy theory kind of wrong in fact. Or there is simply a very big and important piece missing from the puzzle. If de Lorgeril is wrong and the FOURIER mortality numbers not spurious, then we have a huge difference between the risk reduction properties of statin induced LDL reduction and PCSK9i induced LDL reduction, a difference that is already quite expressed, though not statistically significant when comparing an old-data meta analysis for primary prevention with the secondary prevention FOURIER trial data. A difference that is bound to be much more expressed thus for secondary prevention old-data statin results.
Note, I'm not claiming there is evidence that LDL is 100% benign or anything, just that there are major unexplained discrepancies in trial results that MIGHT be explained, either by de Lorgeril being correct about pre-2006 trails, by the fatal CVD event reduction rate of statins being "mostly" unrelated to LDL lowering or by some yet unknown adverse effect of PCSK9i. More research is definitely required. More research and more open raw data sets. As such the main conclusion of this blog post must be that the recent AHA publication on SFA and LDL is in no way based on science that is in any way settled. The science around the LDL hypothesis isn't settled. Not even close. The parts of the puzzle don't fit and until new more conclusive data comes out, or until real hard evidence of mall intend surfaces, no one should not be making any statements that imply settled science on the matter, especially not the AHA. Yes, things are confusing. They should be. Aiming for clarity based on insufficient data in matters like this is a huge gamble. A gamble, potentially with the health and lives of many people affected. A sound that is often heard is that people need clarity, not confusion, but false clarity based on unsettled science can be disastrous. Just be honest AHA and say the words: "We really aren't sure about this one so we stick with the old paradigm until conclusive evidence comes in". People need honest and potentially confusing messages more than they need false clarity.