Human sarcoptosis. (Sarna Humana).
Human sarcoptosis is a highly transmissible, cosmopolitan disease whose etiological agent is the mite Sarcoptes scabiei, of the Arachnida group, of the order Astigmata. Poverty, overcrowding and sexual promiscuity are the most important factors in the transmission. It is associated with low socioeconomic strata in which it is also common to observe poor hygiene and nutrition. It is transmitted mainly by direct, close contact, without discarding the evidence of transmission by fomites (for example, bedding or personnel in severe infestations) and sexual contact. The risk in some institutions (nursing homes, schools, barracks, hospitals) must be taken into account. Dogs and cats and other animals also suffer from parasitism. Pets with S. scabiei var canis may be responsible for infestation and sensitization, causing limited papular dermatitis, although species specificity generally exists. (Wolf et al., 2010).
The adult arthropod (Fig. 1). It measures 1 - 3 mm in length, has a flattened, oval body and 4 pairs of legs. The digestive tract occupies a large proportion of the body. It has a whitish coloration, with the convex back covered with bristles and chitinous spines. There are not two or three eyes that are provided with teeth. The face is short like the legs that have pedicels with or without suction cups. Presentation of spines and dorsal striations with anus. Back-terminal year. Back with sharp scales and short spines.

Biological Cycle Figure one:
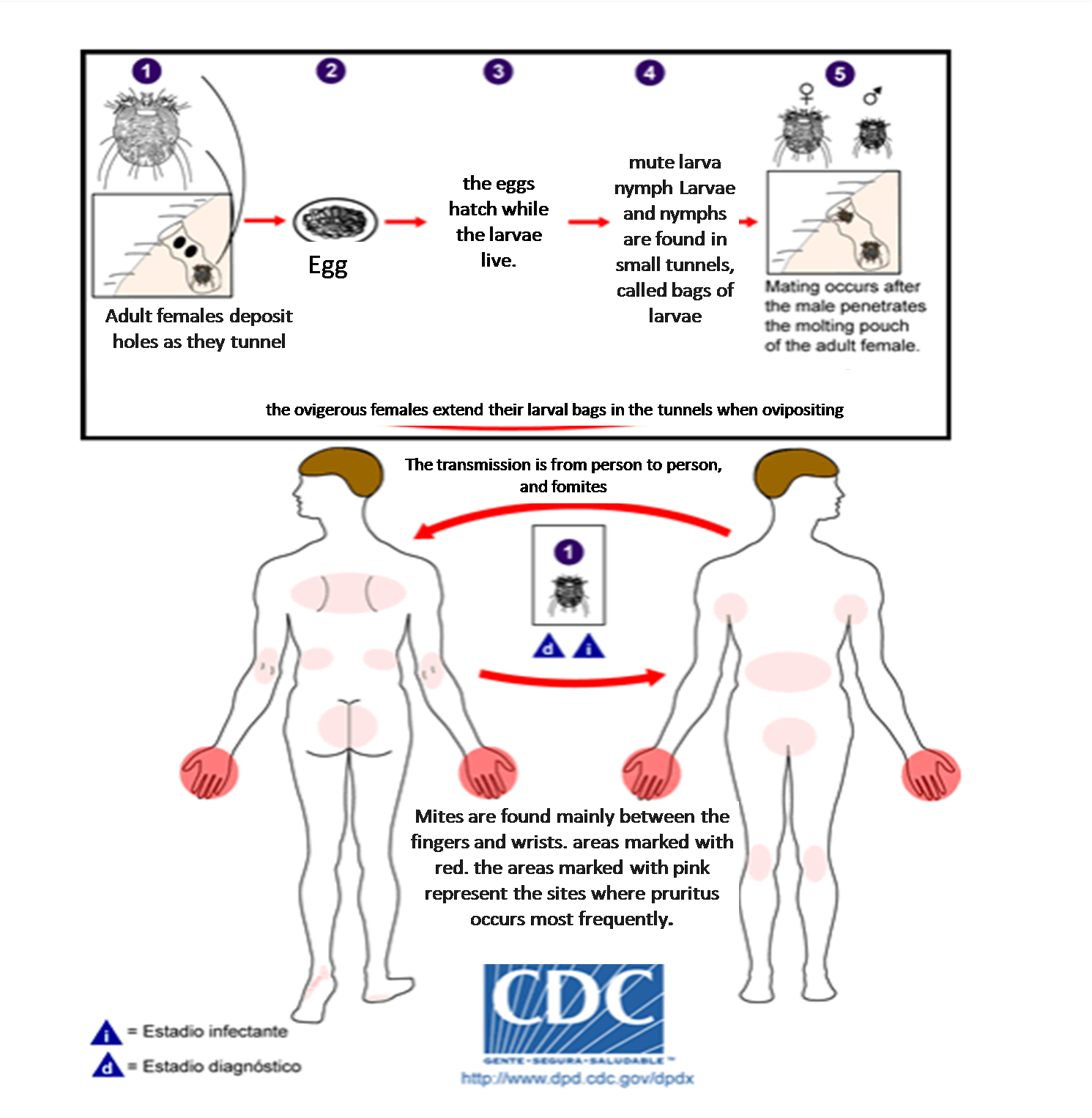
Biological cycle (fig.1). Sarcoptes scabei goes through four stages in its biological cycle; egg, larva, nymph and adult. The females oviposit at intervals of 2 to 3 days making tunnels through the skin. 1: The eggs are oval and from 0.1 to 0.15 mm in length 2: with incubation times of 3 to 8 days. Once the eggs hatch, the larvae migrate to the surface of the skin by piercing the stratum corneum to build almost invisible tunnels, called larval bags. The larval stage, which emerges from the eggs, presents only 3 pairs of legs, 3: this form occurs for 2 to 3 days. After the larva molts, nymphs with 4 pairs of legs are produced. 4: This silent form in slightly larger nymphs before moving adults. Larvae and nymphs can be found in larval bags or hair follicles and look like adults, only they are smaller. Adults are round, like mites like sack without eyes. The females are 0.3 to 0.4 mm long and 0.25 to 0.35 mm wide and the males are slightly less than half this size. The mating takes place after the nomad male penetrates the larval bags of the adult female. 5: The pregnant females extend their larval bags in the characteristic tunnels, carrying the eggs in this process. The pregnant females make tunnels and use their last 2 months of life under the surface of the skin to oviponer. The males are rarely seen, they make runners on the skin before mating. Mites are found predominantly on the fingers and wrists and are attached to the skin by suckers on their previous pair of legs.
Clinical picture (Figure 3):
• It causes itching, very frequent in the hands and particularly in the interdigital spaces (D), wrists, edges of hands and feet, shoulder blades, elbows and knees, penis, scrotum, breast folds and even nipples, buttocks, armpits, waist and popliteal folds.
• In children it can be pruritus on the palms of the hands, soles of the feet, head and neck, with vesicles and pustules. The elderly have few lesions, very pruritic and with an abundance of mites, which can be observed in a scraping of the scales. (C).
• Severe itching often occurs, especially at night and in most parts of the body, including areas where mites do not live.
• Formation of thick crusts (C). They involve hands and feet, grayish scales and scabs on the trunk and extremities, peeling in the facial area, wart-like lesions on fingers and trauma sites, and profuse hair loss. Complications are caused by secondary bacterial infections at the scraping sites.

Diagnosis.
Epidemiological: Similar pictures in the familiar or communal environment, in institutions.
Location of lesions and morphology of the lesions.
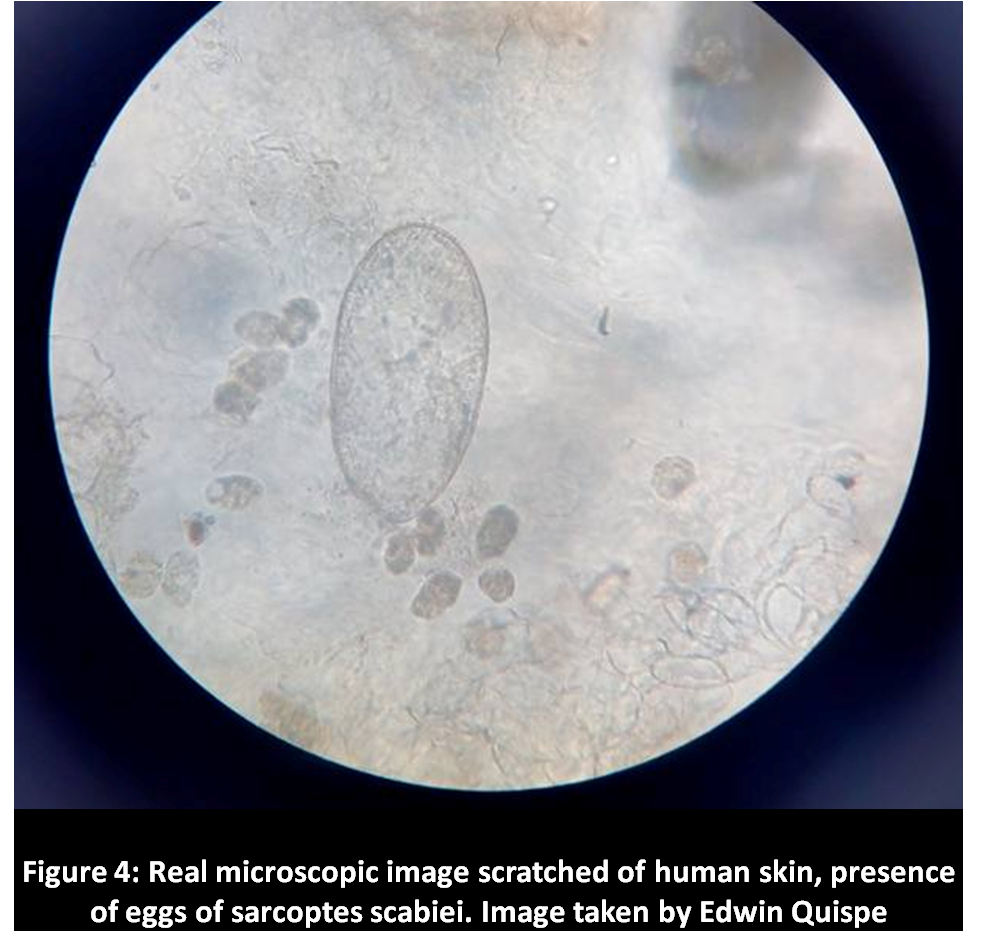
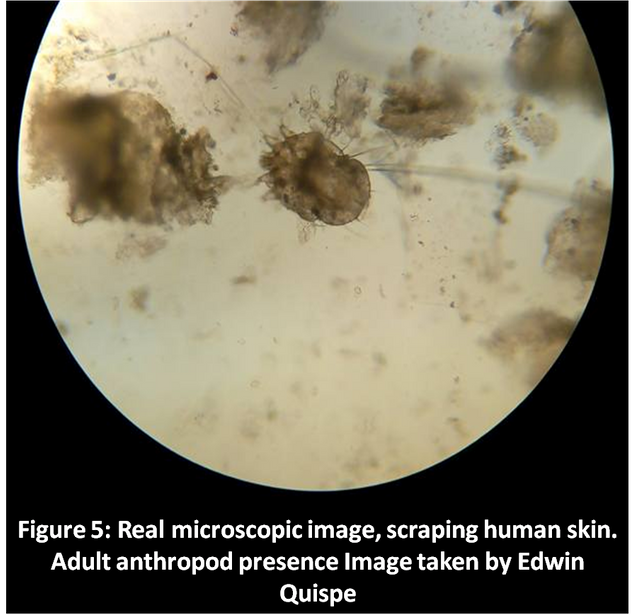
- Skin scraping: observation of the microcoscope of eggs of sarcoptes (fig.4) and presence of an adult anthropod of sarcoptes. Observation of scales.
- Skin biopsy. Inflammatory infiltrate composed of eosinophils, lymphocytes, histiocytes. Larvae, nymphs, females can be observed.
- Useful non-invasive auxiliary tools can be visualization through videodermatoscopy, dermoscopy, confocal microscopy. (Micali et al., 2016).
Treatment:
It must be applied to all family members and close contacts.
It includes personal hygiene and clothes. It is suggested to wash clothes in hot water and store in plastic bags that can not be washed for 2 weeks.
Systemic antibiotics in the treatment of secondary bacterial impetigo and anthistaminics for the control of pruritus.
The single dose of ivermectin is effective.
In severe cases, up to three administrations are recommended, c / 1 - 2 weeks.
Topical agents include: Permethrin cream or 5% emulsion (Scabisan), benzyl benzoate in 25% emulsion for adults (Hastilan), cream crotamiton (Eurax), very effective against pruritus. (Engelman et al., 2013).
reference:
Engelman D, Kiang K, Chosidow O, McCarthy J, Fuller C, et al. Toward the Global Control of Human Scabies: Introducing the International Alliance for the Control of Scabies. PLoS Negl Trop Dis, 2013; 7 (8): e2167. doi: 10.1371 / journal.pntd.0002167.
Micali G, Lacarrubba F, Verzì AE, Chosidow O, Schwartz RA. Scabies: Advances in Noninvasive Diagnosis. PLoS Negl Trop Dis. 2016;10(6): e0004691. doi:10.1371/journal.pntd.0004691.
Mohammad Reza Namazi and Behrooz Barikbin. Atypical Crusted Scabies in an Iranian man. Dermatology Online Journal 8 (2): 17. Clinical case with good images.
Nolan K, Kamrath J, Levitt J. Lindane toxicity: a comprehensive review of the medical literature. Pediatr Dermatol. 2012 Mar-Apr; 29 (2): 141-6. doi: 10.1111 / j.1525-1470.2011.01519.x.
Parasitology program. www.fba.org.ar/panel-gestion/InformeResultado/PA/PA101.pd.
Ronni Wolf R, Batya Davidovici B. Controversies in Dermatology: Part III. Treatment of scabies and pediculosis: Facts and controversies. Clin Dermatol, Sept-Oct 2010; 28 (5): 511-518 http://dx.doi.org/10.1016/j.clindermatol.2010.03.008.